Chlorotrianisene
 | |
| Clinical data | |
|---|---|
| Trade names | Tace |
| AHFS/Drugs.com | Multum Consumer Information |
| Pregnancy category |
|
| Routes of administration | Oral |
| ATC code | G03CA06 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Protein binding | 50 to 80% |
| Identifiers | |
| |
| Synonyms | NSC-10108 |
| CAS Number |
569-57-3 |
| PubChem (CID) | 11289 |
| IUPHAR/BPS | 7146 |
| DrugBank |
DB00269 |
| ChemSpider |
10815 |
| UNII |
6V5034L121 |
| KEGG |
D00269 |
| ChEBI |
CHEBI:3641 |
| ChEMBL |
CHEMBL1200761 |
| ECHA InfoCard | 100.008.472 |
| Chemical and physical data | |
| Formula | C23H21ClO3 |
| Molar mass | 380.864 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
| | |
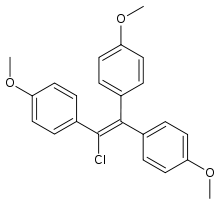
Chlorotrianisene (INN, USAN, BAN; brand names Tace, Estregur, Anisene, Clorotrisin, Merbentyl, Triagen, many others; also known as CTA; tri-p-anisylchloroethylene, TACE, or tris(p-methoxyphenyl)chloroethylene) is a synthetic, non-steroidal estrogen of the triphenylethylene group that was formerly used for the treatment of menopausal symptoms, estrogen deficiency, and prostate cancer before being discontinued.[1][2][3] It was approved in the United States as TACE in 1952, and was introduced throughout Europe subsequently.[4] CTA was the first estrogenic compound of the triphenylethylene series to be introduced.[5]
CTA was derived from estrobin (DBE), a derivative of the very weakly estrogenic compound triphenylethylene (TPE), which in turn was derived from structural modification of diethylstilbestrol (DES).[6][7][8][9] CTA is a relatively weak estrogen, with about one-eighth the potency of DES.[6][7] However, it is highly lipophilic and is stored in fat tissue for prolonged periods of time, with its slow release from fat resulting in a very long duration of action.[6][7][8] CTA itself is inactive; it behaves as a prodrug to a weak estrogen that is formed as a metabolite via degradation of CTA in the liver.[6][10] As such, the potency of CTA is reduced if it is given parenterally instead of orally.[6]
Although it is referred to as a weak estrogen and was used solely as an estrogen in clinical practice, CTA is actually a partial agonist of the estrogen receptor.[7] As such, it is a selective estrogen receptor modulator (SERM), with predominantly estrogenic but also antiestrogenic effects, and was arguably the first SERM to ever be introduced.[5] CTA can antagonize estradiol at the level of the hypothalamus, resulting in disinhibition of the hypothalamic-pituitary-gonadal axis and an increase in estrogen levels.[7] Clomifene and tamoxifen were both derived from CTA via structural modification, and are much weaker partial agonists than CTA and hence much more antiestrogenic in comparison.[7] As an example, chlorotrianisene produces gynecomastia in men,[11] albeit reportedly to a lesser extent than other estrogens,[12] while clomifene and tamoxifen do not and can actually be used to treat gynecomastia.[13]
See also
References
- ↑ J. Elks (14 November 2014). The Dictionary of Drugs: Chemical Data: Chemical Data, Structures and Bibliographies. Springer. pp. 263–. ISBN 978-1-4757-2085-3.
- ↑ Index Nominum 2000: International Drug Directory. Taylor & Francis. January 2000. pp. 219–. ISBN 978-3-88763-075-1.
- ↑ I.K. Morton; Judith M. Hall (6 December 2012). Concise Dictionary of Pharmacological Agents: Properties and Synonyms. Springer Science & Business Media. pp. 73–. ISBN 978-94-011-4439-1.
- ↑ William Andrew Publishing (22 October 2013). Pharmaceutical Manufacturing Encyclopedia, 3rd Edition. Elsevier. pp. 980–. ISBN 978-0-8155-1856-3.
- 1 2 Janos Fischer; C. Robin Ganellin; David P. Rotella (15 October 2012). Analogue-based Drug Discovery III. John Wiley & Sons. pp. 5–. ISBN 978-3-527-65110-8.
- 1 2 3 4 5 A. Wayne Meikle (24 April 2003). Endocrine Replacement Therapy in Clinical Practice. Springer Science & Business Media. pp. 486–. ISBN 978-1-59259-375-0.
- 1 2 3 4 5 6 Walter Sneader (23 June 2005). Drug Discovery: A History. John Wiley & Sons. pp. 198–. ISBN 978-0-471-89979-2.
- 1 2 Jordan VC, Mittal S, Gosden B, Koch R, Lieberman ME (1985). "Structure-activity relationships of estrogens". Environ. Health Perspect. 61: 97–110. doi:10.1289/ehp.856197. PMC 1568776
 . PMID 3905383.
. PMID 3905383. - ↑ Carmen Avendano; J. Carlos Menendez (11 June 2015). Medicinal Chemistry of Anticancer Drugs. Elsevier Science. pp. 87–. ISBN 978-0-444-62667-7.
- ↑ John Hadden (9 November 2013). Pharmacology. Springer Science & Business Media. pp. 249–. ISBN 978-1-4615-9406-2.
- ↑ Jie Jack Li (3 April 2009). Triumph of the Heart: The Story of Statins. Oxford University Press, USA. pp. 34–. ISBN 978-0-19-532357-3.
- ↑ VITAMINS AND HORMONES. Academic Press. 18 May 1976. pp. 387–. ISBN 978-0-08-086630-7.
- ↑ Khan, H. N (2003). "Endocrine treatment of physiological gynaecomastia". BMJ. 327 (7410): 301–302. doi:10.1136/bmj.327.7410.301. ISSN 0959-8138.