Copper in health
Copper is an essential trace element that is vital to the health of all living things (humans, plants, animals, and microorganisms). In humans, copper is essential to the proper functioning of organs and metabolic processes. The human body has complex homeostatic mechanisms which attempt to ensure a constant supply of available copper, while eliminating excess copper whenever this occurs. However, like all essential elements and nutrients, too much or too little nutritional ingestion of copper can result in a corresponding condition of copper excess or deficiency in the body, each of which has its own unique set of adverse health effects.
Daily dietary standards for copper have been set by various health agencies around the world. Standards adopted by some nations recommend different copper intake levels for adults, pregnant women, infants, and children, corresponding to the varying need for copper during different stages of life.
Copper deficiency and toxicity can be either of genetic or non-genetic origin. The study of copper's genetic diseases, which are the focus of intense international research activity, has shed insight into how human bodies use copper, and why it is important as an essential micronutrient. The studies have also resulted in successful treatments for genetic copper excess conditions, enabling patients whose lives were once jeopardized to live long and productive lives.
Researchers specializing in the fields of microbiology, toxicology, nutrition, and health risk assessments are working together to define the precise copper levels that are required for essentiality, while avoiding deficient or excess copper intakes. Results from these studies are expected to be used to fine-tune governmental dietary recommendation programs which are designed to help protect public health.
Essentiality
Copper is an essential trace element (i.e., micronutrient) that is required for plant, animal, and human health.[1] It is also required for the normal functioning of aerobic (oxygen-requiring) microorganisms.
Copper is incorporated into a variety of proteins and metalloenzymes which perform essential metabolic functions; the micronutrient is necessary for the proper growth, development, and maintenance of bone, connective tissue, brain, heart, and many other body organs. Copper is involved in the formation of red blood cells, the absorption and utilization of iron, the metabolism of cholesterol and glucose, and the synthesis and release of life-sustaining proteins and enzymes. These enzymes in turn produce cellular energy and regulate nerve transmission, blood clotting, and oxygen transport.
Copper stimulates the immune system to fight infections, to repair injured tissues, and to promote healing. Copper also helps to neutralize "free-radicals", which can cause severe damage to cells.
Copper's essentiality was first discovered in 1928, when it was demonstrated that rats fed a copper-deficient milk diet were unable to produce sufficient red blood cells.[2] The anemia was corrected by the addition of copper-containing ash from vegetable or animal sources.
As an essential trace element, daily dietary requirements for copper have been recommended by a number of governmental health agencies around the world.
Fetuses, infants, and children
Copper is essential for the normal growth and development of human fetuses, infants, and children.[3] The human fetus accumulates copper rapidly in its liver during the third trimester of pregnancy. At birth, a healthy infant has four times the concentration of copper than a full-grown adult. Human milk is relatively low in copper, and the neonate's liver stores falls rapidly after birth, supplying copper to the fast-growing body during the breast feeding period. These supplies are necessary to carry out such metabolic functions as cellular respiration, melanin pigment and connective tissue synthesis, iron metabolism, free radical defense, gene expression, and the normal functioning of the heart and immune systems in infants.
Infants have special biochemical mechanisms for adequately managing copper in their bodies while permanent lifelong mechanisms develop and mature.[4]
Severe deficiency of copper in pregnant mothers increases the risk of health problems in their fetuses and infants. Health effects noted include low birth weights, muscle weaknesses, and neurologic problems. However, copper deficiencies in pregnant women can be avoided with a balanced diet.
Since copper availability in the body is hindered by an excess of iron and zinc intake, pregnant women prescribed iron supplements to treat anemia or zinc supplements to treat colds should consult physicians to be sure that the prenatal supplements they may be taking also have nutritionally-significant amounts of copper.
When newborn babies are breastfed, the babies' livers and the mothers' breast milk provide sufficient quantities of copper for the first 4–6 months of life.[5] When babies are weaned, a balanced diet should provide adequate sources of copper.
Cow's milk and some older infant formulas are depleted in copper. Most formulas are now fortified with copper to prevent depletion.
Most well-nourished children have adequate intakes of copper. Health-compromised children, including those who are premature, malnourished, have low birth weights, suffer from infections, and who experience rapid catch-up growth spurts, are at elevated risk for copper deficiencies. Fortunately, diagnosis of copper deficiency in children is clear and reliable once the condition is suspected. Supplements under a physician's supervision usually facilitate a full recovery.
Homeostasis
Copper is absorbed, transported, distributed, stored, and excreted in the body according to complex homeostatic processes which ensure a constant and sufficient supply of the micronutrient while simultaneously avoiding excess levels.[1] If an insufficient amount of copper is ingested for a short period of time, copper stores in the liver will be depleted. Should this depletion continue, a copper health deficiency condition may develop. If too much copper is ingested, an excess condition can result. Both of these conditions, deficiency and excess, can lead to tissue injury and disease. However, due to homeostatic regulation, the human body is capable of balancing a wide range of copper intakes for the needs of healthy individuals.[6]
Many aspects of copper homeostasis are known at the molecular level.[7][8] Copper's essentiality is due to its ability to act as an electron donor or acceptor as its oxidation state fluxes between Cu1+(cuprous) and Cu2+ (cupric).[3] As a component of about a dozen cuproenzymes, copper is involved in key redox (i.e., oxidation-reduction) reactions in essential metabolic processes such as mitochondrial respiration, synthesis of melanin, and cross-linking of collagen.[9] Copper is an integral part of the antioxidant enzyme, copper-zinc superoxide dismutase (Cu,Zn-SOD), and has a role in iron homeostasis as a cofactor in ceruloplasmin.[3] A list of some key copper-containing enzymes and their functions is summarized below:
| Enzymes | Function |
|---|---|
| Amine oxidases | Group of enzymes oxidizing primary amines (e.g., tyramine, histidine and polylamines) |
| Ceruloplasmin (ferroxidase I) | Multi-copper oxidase in plasma, essential for iron transport |
| Cytochrome c oxidase | Terminal oxidase enzyme in mitochondrial respiratory chain, involved in electron transport |
| Dopamine β-hydroxylase | Involved in catecholamine metabolism, catalyzes conversion of dopamine to norepinephrine |
| Hephaestin | Multi-copper ferroxidase, involved in iron transport across intestinal mucosa into portal circulation |
| Lysyl oxidase | Cross-linking of collagen and elastin |
| Peptidylglycine alpha-amidating mono-oxygenase (PAM) | Multifunction enzyme involved in maturation and modification of key neuropeptides (e.g., neurotransmitters, neuroendocrine peptides) |
| Superoxide dismutase (Cu, Zn) | Intracellular and extracellular enzyme involved in defense against reactive oxygen species (e.g., destruction of superoxide radicals) |
| Tyrosinase | Enzyme catalyzing melanin and other pigment production |
The transport and metabolism of copper in living organisms is currently the subject of much active research. Copper transport at the cellular level involves the movement of extracellular copper across the cell membrane and into the cell by specialized transporters.[8] In the bloodstream, copper is carried throughout the body by albumin, ceruloplasmin, and other proteins. The majority of blood copper (or serum copper) is bound to ceruloplasmin. The proportion of ceruloplasmin-bound copper can range from 70-95% and differs between individuals, depending, for example, on hormonal cycle, season, and copper status. Intracellular copper is routed to sites of synthesis of copper-requiring enzymes and to organelles by specialized proteins called metallochaperones.[10][11][12] Another set of these transporters carries copper into subcellular compartments.[12][13] Certain mechanisms exist to release copper from the cell. Specialized transporters return excess unstored copper to the liver for additional storage and/or biliary excretion.[10][11] These mechanisms ensure that free unbound toxic ionic copper is unlikely to exist in the majority of the population (i.e., those without genetic copper metabolism defects).
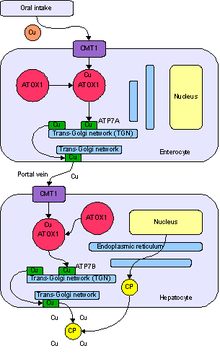
Copper is imported into cells through the cell wall by the plasma membrane transport protein known as Copper Transporter 1, or Ctr1. Ctr1 rapidly binds to intracellular copper chaperone proteins. Atox1 delivers copper to the secretory pathway and docks with either copper-transporting ATPase ATP7B in the liver or ATP7A in other cells. ATP7B directs copper to plasma ceruloplasmin or to biliary excretion in concert with a newly discovered chaperone, Murr1, the protein missing in canine copper toxicosis. ATP7A directs copper within the trans-Golgi network to the proteins dopamine beta-monooxygenase, peptidylglycine alpha-amidating monooxygenase, lysyl oxidase, and tyrosinase, depending on the cell type. CCS is the copper chaperone for the Cu/Zn-superoxide dismutase that protects cells against reactive oxygen species; it delivers copper in the cytoplasm and intermitochondrial space. Cox17 delivers copper to mitochondria to cytochrome c oxidase via the chaperones Cox11, Sco1, and Sco2. Other copper chaperones may exist and might include metallothionein and amyloid precursor protein (APP).[7][8] Genetic and nutritional studies have illustrated the essential nature of these copper-binding proteins.[14]
Absorption
In mammals copper is absorbed in the stomach and small intestine, although there appear to be differences among species with respect to the site of maximal absorption.[15] Copper is absorbed from the stomach and duodenum in rats[16] and from the lower small intestine in hamsters.[17] The site of maximal copper absorption is not known for humans, but is assumed to be the stomach and upper intestine because of the rapid appearance of Cu64 in the plasma after oral administration.[18]
Absorption of copper ranges from 15–97%, depending on copper content, form of the copper, and composition of the diet.[19][20][21][22][23]
Various factors influence copper absorption. For example, copper absorption is enhanced by ingestion of animal protein, citrate, and phosphate. Copper salts, including copper gluconate, copper acetate, or copper sulfate, are more easily absorbed than copper oxides.[24][25] Elevated levels of dietary zinc, as well as cadmium, high intakes of phytate and simple sugars (fructose, sucrose) inhibit dietary absorption of copper.[26][27][28][29][30][31] Furthermore, low levels of dietary copper inhibit iron absorption.
Some forms of copper are not soluble in stomach acids and cannot be absorbed from the stomach or small intestine. Also, some foods may contain indigestible fiber that binds with copper. High intakes of zinc can significantly decrease copper absorption. Extreme intakes of Vitamin C or iron can also affect copper absorption, reminding us of the fact that micronutrients need to be consumed as a balanced mixture. This is one reason why extreme intakes of any one single micronutrient are not advised.[32] Individuals with chronic digestive problems may be unable to absorb sufficient amounts of copper, even though the foods they eat are copper-rich.
Several copper transporters have been identified that can move copper across cell membranes.[33][34] Other intestinal copper transporters may exist. Intestinal copper uptake may be catalyzed by Ctr1. Ctr1 is expressed in all cell types so far investigated, including enterocytes, and it catalyzes the transport of Cu+1 across the cell membrane.[35]
Excess copper (as well as other heavy metal ions like zinc or cadmium) may be bound by metallothionein and sequestered within intracellular vesicles of enterocytes (i.e., predominant cells in the small intestinal mucosa).
Distribution
Copper released from intestinal cells moves to the serosal (i.e., thin membrane lining) capillaries where it binds to albumin, glutathione, and amino acids in the portal blood.[36][37] There is also evidence for a small protein, transcuprein, with a specific role in plasma copper transport[38] Several or all of these copper-binding molecules may participate in serum copper transport. Copper from portal circulation is primarily taken up by the liver. Once in the liver, copper is either incorporated into copper-requiring proteins, which are subsequently secreted into the blood. Most of the copper (70 – 95%) excreted by the liver is incorporated into ceruloplasmin, the main copper carrier in blood. Copper is transported to extra-hepatic tissues by ceruloplasmin,[39] albumin and amino acids, or excreted into the bile.[3] By regulating copper release, the liver exerts homeostatic control over extrahepatic copper.[11]
Excretion
Bile is the major pathway for the excretion of copper and is vitally important in the control of liver copper levels.[40][41][42] Most fecal copper results from biliary excretion; the remainder is derived from unabsorbed copper and copper from desquamated mucosal cells.
| Dose range | Approximate daily intakes | Health outcomes |
|---|---|---|
| Death | ||
| Gross dysfunction and disturbance of metabolism of other nutrients; hepatic
"detoxification" and homeostasis overwhelmed | ||
| Toxic | >5.0 mg/kg body weight | Gastrointestinal metallothionein induced (possible differing effects of acute and chronic
exposure) |
| 100 μg/kg body weight | Plateau of absorption maintained; homeostatic mechanisms regulate absorption of copper | |
| Adequate | 34 μg/kg body weight | Hepatic uptake, sequestration and excretion effect homeostasis; glutathione-dependent uptake of copper; binding to metallothionein; and lysosomal excretion of copper |
| 11 μg/kg body weight | Biliary excretion and gastrointestinal uptake normal | |
| 9 μg/kg body weight | Hepatic deposit(s) reduced; conservation of endogenous copper; gastrointestinal
absorption increased | |
| Deficient | 8.5 μg/kg body weight | Negative copper balance |
| 5.2 μg/kg body weight | Functional defects, such as lysyl oxidase and superoxide dismutase activities reduced; impaired substrate metabolism | |
| 2 μg/kg body weight | Peripheral pools disrupted; gross dysfunction and disturbance of metabolism of other
nutrients; death |
Daily dietary copper requirements
Various national and international organizations concerned with nutrition and health have standards for copper intake at levels judged to be adequate for maintaining good health. These standards, or dietary reference values, are periodically changed and updated as new scientific data become available. The standards sometimes differ among regions and organizations.
Adults
The World Health Organization recommends a minimal acceptable intake of approximately 1.3 mg/day.[44] These values are considered to be adequate and safe for most of the general population. In North America, the recommended intake of copper for healthy adult men and women is 900 micrograms/day (0.9 mg/day).[45][46][47] Health benefits above the recommended adequate intake of 0.9 - 1.3 mg/day have not been established.
In North America, a maximum tolerable intake has been established at 10 mg/day. This is the highest level of copper intake that is not likely to pose a health risk to most adults in the general population. However, this daily intake level is not recommended by any authority.
Adolescents, children, and infants
The World Health Organization has not developed minimum daily intakes for these age groups. In North America, safe and acceptable daily intakes have been estimated from adult data and are as follows: 340 micrograms/day (0.34 mg/day) for children of 1–3 years; 440 micrograms/day (0.44 mg/day) for 4–8 years; 700 micrograms/day (0.7 mg/day) for 9–13 years; and 890 micrograms/day (0.89 mg/day) for 14–18 years.[45][46][47]
In North America, tolerable intakes for these age groups (i.e., intakes not likely to pose a health risk for most children in the general population, but for which no additional health benefits are known) are: 1 mg/day for children of 1–3 years; 3 mg/day for 4–8 years; 5 mg/day for 9–13 years; and 8 mg/day for 14–18 years.
Full-term and premature infants are more sensitive to copper deficiency than adults. Since the fetus accumulates copper during the last 3 months of pregnancy, infants that are born prematurely have not had sufficient time to store adequate reserves of copper in their livers and therefore require more copper at birth than full-term infants.
For full-term infants, the North American recommended safe and adequate intake is approximately 0.2 mg/day. For premature babies, it is considerably higher: 1 mg/day. The World Health Organization has recommended similar minimum adequate intakes and advises that premature infants be given formula supplemented with extra copper to prevent the development of copper deficiency.[32]
Pregnant women and mothers who breastfeed
Nature has devised a way for the fetus to get copper from the mother via the placenta and for infants to get copper via breast milk. For these reasons, pregnancy and nursing increase the body's need for copper. The recommended oral intake in pregnant and nursing women is slightly higher than for non-pregnant, non-nursing healthy women (approximately 1 mg/day for pregnant women and 1.3 mg/day for nursing mothers aged 14–50 years).[32]
The best source of copper and other essential micronutrients during the first year of life is human milk. If a full-term infant is not nursed, fortified baby formula is highly recommended. Cow's milk, however, contains very low amounts of bioavailable copper and should be supplemented with copper during the first year of life.
Dietary sources

Copper is an essential trace mineral that cannot be formed by the human body. It must be ingested from dietary sources.
Foods contribute virtually all of the copper consumed by humans.[48][49][50] The best dietary sources include seafood (especially shellfish), organ meats (e.g., liver), whole grains, legumes (e.g., beans and lentils) and chocolate. Nuts, including peanuts and pecans, are especially rich in copper, as are grains such as wheat and rye, and several fruits including lemons and raisins. Other food sources that contain copper include cereals, potatoes, peas, red meat, mushrooms, some dark green leafy vegetables (such as kale), and fruits (coconuts, papaya and apples). Tea, rice and chicken are relatively low in copper, but can provide a reasonable amount of copper when they are consumed in significant amounts.
Eating a balanced diet with a range of foods from different food groups is the best way to avoid copper deficiency. In both developed and developing countries, adults, young children, and adolescents who consume diets of grain, millet, tuber, or rice along with legumes (beans) or small amounts of fish or meat, some fruits and vegetables, and some vegetable oil are likely to obtain adequate copper if their total food consumption is adequate in calories. In developed countries where consumption of red meat is high, copper intake is also likely to be adequate.
As a natural element in the earth's crust, copper exists in most of the world's surface water and groundwater, although the actual concentration of copper in natural waters varies geographically. Drinking water can comprise 20-25% of dietary copper.[51]
In many regions of the world, copper tubing that conveys drinking water can be a source of dietary copper. Copper tube can leach a small amount of copper, particularly in its first year or two of service. Afterwards, a protective surface usually forms on the inside of copper tubes that retards leaching.
Supplementation
Copper supplements can prevent copper deficiency, but supplements should be taken only under a doctor's supervision. Different forms of copper supplementation have different absorption rates. For example, the absorption of copper from cupric oxide supplements is lower than that from copper gluconate, sulfate, or carbonate.
Supplementation is generally not recommended for healthy adults who consume a well-balanced diet which includes a wide range of foods. However, supplementation under the care of a physician may be necessary for premature infants or those with low birth weights, infants fed unfortified formula or cow's milk during the first year of life, and malnourished young children. Physicians may consider copper supplementation for 1) illnesses that reduce digestion (e.g., children with frequent diarrhea or infections; alcoholics), 2) insufficient food consumption (e.g., the elderly, the infirm, those with eating disorders or on diets), 3) patients taking medications that block the body's use of copper, 4) anemia patients who are treated with iron supplements, 5) anyone taking zinc supplements, and 6) those suffering from osteoporosis.
Many popular vitamin supplements include copper as small inorganic molecules such as cupric oxide. These supplements can result in excess free copper in the brain as the copper can cross the blood-brain barrier directly. Normally, organic copper in food is first processed by the liver which keeps free copper levels under control.
Copper deficiency and excess health conditions (non-genetic)
If insufficient quantities of copper are ingested, copper reserves in the liver will become depleted and a copper deficiency leading to disease or tissue injury (and in extreme cases, death). Toxicity from copper deficiency can be treated with a balanced diet or supplementation under the supervision of a doctor. On the contrary, like all substances, excess copper intake at levels far above World Health Organization limits can become toxic.[52] Acute copper toxicity is generally associated with accidental ingestion. These symptoms abate when the high copper food source is no longer ingested.
In 1996, the International Program on Chemical Safety, a World Health Organization-associated agency, stated "there is greater risk of health effects from deficiency of copper intake than from excess copper intake." This conclusion was confirmed in recent multi-route exposure surveys.[49][53]
The health conditions of non-genetic copper deficiency and copper excess are described below.
Copper deficiency
A number of nutrition surveys have indicated that the diets of approximately 25% of adolescents, adults, and people over 65, do not meet the recommended daily nutrient intake for copper.[7] These studies also suggest that long-term acquired copper deficiency is under-diagnosed and is much more common than suspected.
Acquired copper deficiency has recently been implicated in adult-onset progressive myeloneuropathy[54] and in the development of severe blood disorders including myelodysplastic syndrome.[8][55][56] Fortunately, copper deficiency can be confirmed by very low serum metal and ceruloplasmin concentrations in the blood.
Other conditions previously linked to copper deficiency include osteoporosis, osteoarthritis, rheumatoid arthritis, cardiovascular disease, colon cancer, and chronic conditions involving bone, connective tissue, heart, and blood vessels.[7][57][58][59][60]
Copper deficiency alters the role of other cellular constituents involved in antioxidant activities, such as iron, selenium, and glutathione, and therefore plays an important role in diseases in which oxidant stress is elevated.[51][61][62]
In both humans and animals, the major target organs for copper deficiency are the blood and hematopoietic system, the cardiovascular system, connective tissue and bone, the nervous system, and the immune system.[3][9][58]
A marginal (i.e., 'mild') copper deficiency, believed to be more widespread than previously thought, can impair human health in subtle ways.[51] Those affected suffer from lowered resistance to infection, general fatigue, impaired neurological function, and elevated risk for coronary heart disease and osteoporosis.
Populations susceptible to copper deficiency include those with genetic defects for Menkes disease, low-birth-weight infants, infants fed cow's milk instead of breast milk or fortified formula, pregnant and lactating mothers, patients receiving total parenteral nutrition, individuals with "malabsorption syndrome" (impaired dietary absorption), diabetics, individuals with chronic diseases that result in low food intake, such as alcoholics, and persons with eating disorders. The elderly and athletes may also be at higher risk for copper deficiency due to special needs that increase the daily requirements.[31] Vegetarians may have decreased copper intake due to the consumption of plant foods in which copper bioavailability is low.[28][63][64] Fetuses and infants of severely copper deficient women have increased risk of low birth weights, muscle weaknesses, and neurological problems. Copper deficiencies in these populations may result in anemia, bone abnormalities, impaired growth, weight gain, frequent infections (colds, flu, pneumonia), poor motor coordination, and low energy.
Copper excess
Copper excess is a subject of much current research. Distinctions have emerged from studies that copper excess factors are different in normal populations versus those with increased susceptibility to adverse effects and those with rare genetic diseases.[9][51] This has led to statements from health organizations that could be confusing to the uninformed. For example, according to a U.S. Institute of Medicine report,[46] the intake levels of copper for a significant percentage of the population are lower than recommended levels. On the other hand, the U.S. National Research Council[65] concluded in its report Copper in Drinking Water that there is concern for copper toxicity in susceptible populations and recommended that additional research be conducted to identify and characterize copper-sensitive populations.
Excess copper intake causes stomach upset, nausea, and diarrhea and can lead to tissue injury and disease.
The oxidation potential of copper may be responsible for some of its toxicity in excess ingestion cases. At high concentrations copper is known to produce oxidative damage to biological systems, including peroxidation of lipids or other macromolecules.[66]
While the cause and progression of Alzheimer's disease are not well understood, research indicates that, among several other key observations, iron,[67][68] aluminum,[69] and copper[70][71] accumulate in the brains of Alzheimer's patients. However, it is not yet known whether this accumulation is a cause or a consequence of the disease.
Research has been ongoing over the past two decades to determine whether copper is a causative or a preventive agent of Alzheimer's disease. For example, as a possible causative agent or an expression of a metal homeostasis disturbance, studies indicate that copper may play a role in increasing the growth of protein clumps in Alzheimer's disease brains,[72] possibly by damaging a molecule that removes the toxic buildup of amyloid beta (Aβ) in the brain.[73] There is an association between a diet rich in copper and iron together with saturated fat and Alzheimer's disease.[74] On the other hand, studies also demonstrate potential beneficial roles of copper in treating rather than causing Alzheimer's disease.[75] For example, copper has been shown to 1) promote the non-amyloidogenic processing of amyloid beta precursor protein (APP), thereby lowering amyloid beta (Aβ) production in cell culture systems 2) increase lifetime and decrease soluble amyloid production in APP transgenic mice, and 3) lower Aβ levels in cerebral spinal fluid in Alzheimer's disease patients.[76]
Furthermore, long-term copper treatment (oral intake of 8 mg copper (Cu-(II)-orotate-dihydrate)) was excluded as a risk factor for Alzheimer's disease in a noted clinical trial on humans[77] and a potentially beneficial role of copper in Alzheimer's disease has been demonstrated on cerebral spinal fluid levels of Aβ42, a toxic peptide and biomarker of the disease.[78] More research is needed to understand metal homeostasis disturbances in Alzheimer's disease patients and how to address these disturbances therapeutically. Since this experiment used Cu-(II)-orotate-dihydrate, it does not relate to the effects of cupric oxide in supplements.[79]
Copper toxicity from excess exposures
In humans, the liver is the primary organ of copper-induced toxicity. Other target organs include bone and the central nervous and immune systems.[9] Excess copper intake also induces toxicity indirectly by interacting with other nutrients. For example, excess copper intake produces anemia by interfering with iron transport and/or metabolism.[3][9]
The identification of genetic disorders of copper metabolism leading to severe copper toxicity (i.e., Wilson disease) has spurred research into the molecular genetics and biology of copper homeostasis (for further information, refer to the following section on copper genetic diseases). Much attention has focused on the potential consequences of copper toxicity in normal and potentially susceptible populations. Potentially susceptible subpopulations include hemodialysis patients and individuals with chronic liver disease. Recently, concern was expressed about the potential sensitivity to liver disease of individuals who are heterozygote carriers of Wilson disease genetic defects (i.e., those having one normal and one mutated Wilson copper ATPase gene) but who do not have the disease (which requires defects in both relevant genes).[80] However, to date, no data are available that either support or refute this hypothesis.
Acute exposures
In case reports of humans intentionally or accidentally ingesting high concentrations of copper salts (doses usually not known but reported to be 20–70 grams of copper), a progression of symptoms was observed including abdominal pain, headache, nausea, dizziness, vomiting and diarrhea, tachycardia, respiratory difficulty, hemolytic anemia, hematuria, massive gastrointestinal bleeding, liver and kidney failure, and death.
Episodes of acute gastrointestinal upset following single or repeated ingestion of drinking water containing elevated levels of copper (generally above 3–6 mg/L) are characterized by nausea, vomiting, and stomach irritation. These symptoms resolve when copper in the drinking water source is reduced.
Three experimental studies were conducted that demonstrate a threshold for acute gastrointestinal upset of approximately 4–5 mg/L in healthy adults, although it is not clear from these findings whether symptoms are due to acutely irritant effects of copper and/or to metallic, bitter, salty taste.[81][82][83][84] In an experimental study with healthy adults, the average taste threshold for copper sulfate and chloride in tap water, deionized water, or mineral water was 2.5–3.5 mg/L.[85] This is just below the experimental threshold for acute gastrointestinal upset.
Chronic exposures
The long-term toxicity of copper has not been well studied in humans, but it is infrequent in normal populations that do not have a hereditary defect in copper homeostasis.[86]
There is little evidence to indicate that chronic human exposure to copper results in systemic effects other than liver injury.[65] Chronic copper poisoning leading to liver failure was reported in a young adult male with no known genetic susceptibility who consumed 30–60 mg/d of copper as a mineral supplement for 3 years.[87] Individuals residing in U.S. households supplied with tap water containing >3 mg/L of copper exhibited no adverse health effects.[88]
No effects of copper supplementation on serum liver enzymes, biomarkers of oxidative stress, and other biochemical endpoints have been observed in healthy young human volunteers given daily doses of 6 to 10 mg/d of copper for up to 12 weeks.[89][90][91][92] Infants aged 3–12 months who consumed water containing 2 mg Cu/L for 9 months did not differ from a concurrent control group in gastrointestinal tract (GIT) symptoms, growth rate, morbidity, serum liver enzyme and bilirubin levels, and other biochemical endpoints.[93]) Serum ceruloplasmin was transiently elevated in the exposed infant group at 9 months and similar to controls at 12 months, suggesting homeostatic adaptation and/or maturation of the homeostatic response.[8]
Dermal exposure has not been associated with systemic toxicity but anecdotal reports of allergic responses may be a sensitization to nickel and cross-reaction with copper or a skin irritation from copper.[9] Workers exposed to high air levels of copper (resulting in an estimated intake of 200 mg Cu/d) developed signs suggesting copper toxicity (e.g., elevated serum copper levels, hepatomegaly). However, other co-occurring exposures to pesticidal agents or in mining and smelting may contribute to these effects.[9] Effects of copper inhalation are being thoroughly investigated by an industry-sponsored program on workplace air and worker safety. This multi-year research effort is expected to be finalized in 2011.
Measurements of elevated copper status
Although a number of indicators are useful in diagnosing copper deficiency, there are no reliable biomarkers of copper excess resulting from dietary intake. The most reliable indicator of excess copper status is liver copper concentration. However, measurement of this endpoint in humans is intrusive and not generally conducted except in cases of suspected copper poisoning. Increased serum copper or ceruolplasmin levels are not reliably associated with copper toxicity as elevations in concentrations can be induced by inflammation, infection, disease, malignancies, pregnancy, and other biological stressors. Levels of copper-containing enzymes, such as cytochrome c oxidase, superoxide dismutase, and diaminase oxidase, vary not only in response to copper state but also in response to a variety of other physiological and biochemical factors and therefore are inconsistent markers of excess copper status.[94]
A new candidate biomarker for copper excess as well as deficiency has emerged in recent years. This potential marker is a chaperone protein, which delivers copper to the antioxidant protein SOD1 (copper, zinc superoxide dismutase). It is called "copper chaperone for SOD1" (CCS), and excellent animal data supports its use as a marker in accessible cells (e.g., erythrocytes) for copper deficiency as well as excess. CCS is currently being tested as a biomarker in humans.
Hereditary copper metabolic diseases
Several rare genetic diseases (Wilson disease, Menkes disease, idiopathic copper toxicosis, Indian childhood cirrhosis) are associated with the improper utilization of copper in the body.[95] All of these diseases involve mutations of genes containing the genetic codes for the production of specific proteins involved in the absorption and distribution of copper. When these proteins are dysfunctional, copper either builds up in the liver or the body fails to absorb copper.
These diseases are inherited and cannot be acquired. Adjusting copper levels in the diet or drinking water will not cure these conditions (although therapies are available to manage symptoms of genetic copper excess disease).
The study of genetic copper metabolism diseases and their associated proteins are enabling scientists to understand how human bodies use copper and why it is important as an essential micronutrient.
The diseases arise from defects in two similar copper pumps, the Menkes and the Wilson Cu-ATPases.[8] The Menkes ATPase is expressed in tissues like skin-building fibroblasts, kidneys, placenta, brain, gut and vascular system, while the Wilson ATPase is expressed mainly in the liver, but also in mammary glands and possibly in other specialized tissues.[9] This knowledge is leading scientists towards possible cures for genetic copper diseases.[52]
Menkes disease
Menkes disease, a genetic condition of copper deficiency, was first described by John Menkes in 1962. It is a rare X-linked disorder that affects approximately 1/200,000 live births, primarily boys.[7] Livers of Menkes disease patients cannot absorb essential copper needed for patients to survive. Death usually occurs in early childhood: most affected individuals die before the age of 10 years, although several patients have survived into their teens and early 20s.[96]
The protein produced by the Menkes gene is responsible for transporting copper across the gastrointestinal tract (GIT) mucosa and the blood–brain barrier.[8][96] Mutational defects in the gene encoding the copper ATPase cause copper to remain trapped in the lining of the small intestine. Hence, copper cannot be pumped out of the intestinal cells and into the blood for transport to the liver and consequently to rest of the body.[96][97] The disease therefore resembles a severe nutritional copper deficiency despite adequate ingestion of copper.
Symptoms of the disease include coarse, brittle, depigmented hair and other neonatal problems, including the inability to control body temperature, mental retardation, skeletal defects, and abnormal connective tissue growth.
Menkes patients exhibit severe neurological abnormalities, apparently due to the lack of several copper-dependent enzymes required for brain development,[51][98] including reduced cytochrome c oxidase activity.[96] The brittle, kinky hypopigmented hair of steely appearance is due to a deficiency in an unidentified cuproenzyme. Reduced lysyl oxidase activity results in defective collagen and elastin polymerization and corresponding connective-tissue abnormalities including aortic aneurisms, loose skin, and fragile bones.
With early diagnosis and treatment consisting of daily injections of copper histidine intraperitoneally and intrathecally to the central nervous system, some of the severe neurological problems may be avoided and survival prolonged. However, Menkes disease patients retain abnormal bone and connective-tissue disorders and show mild to severe mental retardation.[97] Even with early diagnosis and treatment, Menkes disease is usually fatal.
Ongoing research into Menkes disease is leading to a greater understanding of copper homeostasis,[71] the biochemical mechanisms involved in the disease, and possible ways to treat it.[99] Investigations into the transport of copper across the blood/brain barrier, which are based on studies of genetically altered mice, are designed to help researchers understand the root cause of copper deficiency in Menkes disease. The genetic makeup of "transgenic mice" is altered in ways that help researchers garner new perspectives about copper deficiency. The research to date has been valuable: genes can be 'turned off' gradually to explore varying degrees of deficiency.
Researchers have also demonstrated in test tubes that damaged DNA in the cells of a Menkes patient can be repaired. In time, the procedures needed to repair damaged genes in the human body may be found.
Wilson's disease
Wilson's disease is a rare autosomal (chromosome 13) recessive genetic disorder of copper transport that causes an excess of copper to build up in the liver.[71][100][101] This results in liver toxicity, among other symptoms.[102] The disease is now treatable.
Wilson's disease is produced by mutational defects of a protein that transports copper from the liver to the bile for excretion.[71] The disease involves poor incorporation of copper into ceruloplasmin and impaired biliary copper excretion and is usually induced by mutations impairing the function of the Wilson copper ATPase. These genetic mutations produce copper toxicosis due to excess copper accumulation, predominantly in the liver and brain and, to a lesser extent, in kidneys, eyes, and other organs.
The disease, which affects about 1/30,000 infants of both genders,[9] may become clinically evident at any time from infancy through early adulthood. The age of onset of Wilson's disease ranges from 3 to 50 years of age. Initial symptoms include hepatic, neurologic, or psychiatric disorders and, rarely, renal, skeletal, or endocrine symptomatology. The disease progresses with deepening jaundice and the development of encephalopathy, severe clotting abnormalities, occasionally associated with intravascular coagulation, and terminal renal insufficiency. A peculiar type of tremor in the upper extremities, slowness of movement, and changes in temperament become apparent. Kayser-Fleischer rings, a rusty brown discoloration at the outer rims of the iris due to copper deposition noted in 90% of patients, become evident as copper begins to accumulate and affect the nervous system.[103]
Almost always, death occurs if the disease is untreated.[51] Fortunately, identification of the mutations in the Wilson ATPase gene underlying most cases of Wilson's disease has made DNA testing for diagnosis possible.
If diagnosed and treated early enough, patients with Wilson's disease may live long and productive lives.[99] Wilson's disease is managed by copper chelation therapy with D-penicillamine (which picks up and binds copper and enables patients to excrete excess copper accumulated in the liver), therapy with zinc sulfate or zinc acetate, and restrictive dietary metal intake, such as the elimination of chocolate, oysters, and mushrooms.[51] Zinc therapy is now the treatment of choice. Zinc produces a mucosal block by inducing metallothionein, which binds copper in mucosal cells until they slough off and are eliminated in the feces.[104] and it competes with copper for absorption in the intestine by DMT1 (Divalent Metal transporter 1). More recently, experimental treatments with tetrathiomolybdate showed promising results. Tetrathiomolybdate appears to be an excellent form of initial treatment in patients who have neurologic symptoms. In contrast to penicillamine therapy, initial treatment with tetrathiomolybdate rarely allows further, often irreversible, neurologic deterioration.[105]
Over 100 different genetic defects leading to Wilson's disease have been described and are available on the Internet at . Some of the mutations have geographic clustering.[106]
Many Wilson's patients carry different mutations on each chromosome 13 (i.e., they are compound heterozygotes).[51] Even in individuals who are homozygous for a mutation, onset and severity of the disease may vary.[103][107] Individuals homozygous for severe mutations (e.g., those truncating the protein) have earlier disease onset. Disease severity may also be a function of environmental factors, including the amount of copper in the diet or variability in the function of other proteins that influence copper homeostasis.
It has been suggested that heterozygote carriers of the Wilson's disease gene mutation may be potentially more susceptible to elevated copper intake than the general population.[65] A heterozygotic frequency of 1/90 people has been estimated in the overall population.[9] However, there is no evidence to support this speculation.[8] Further, a review of the data on single-allelic autosomal recessive diseases in humans does not suggest that heterozygote carriers are likely to be adversely affected by their altered genetic status.
Other copper-related hereditary syndromes
Other diseases in which abnormalities in copper metabolism appear to be involved include Indian childhood cirrhosis (ICC), endemic Tyrolean copper toxicosis (ETIC), and idiopathic copper toxicosis (ICT), also known as non-Indian childhood cirrhosis. ICT is a genetic disease recognized in the early twentieth century primarily in the Tyrolean region of Austria and in the Pune region of India.[51]
ICC, ICT, and ETIC are infancy syndromes that are similar in their apparent etiology and presentation.[108] Both appear to have a genetic component and a contribution from elevated copper intake.
In cases of ICC, the elevated copper intake is due to heating and/or storing milk in copper or brass vessels. ICT cases, on the other hand, are due to elevated copper concentrations in water supplies.[9][109] Although exposures to elevated concentrations of copper are commonly found in both diseases, some cases appear to develop in children who are exclusively breastfed or who receive only low levels of copper in water supplies.[109] The currently prevailing hypothesis is that ICT is due to a genetic lesion resulting in impaired copper metabolism combined with high copper intake. This hypothesis was supported by the frequency of occurrence of parental consanguinity in most of these cases, which is absent in areas with elevated copper in drinking water and in which these syndromes do not occur.[109]
ICT appears to be vanishing as a result of greater genetic diversity within the affected populations in conjunction with educational programs to ensure that tinned cooking utensils are used instead of copper pots and pans being directly exposed to cooked foods. The preponderance of cases of early childhood cirrhosis identified in Germany over a period of 10 years were not associated with either external sources of copper or with elevated hepatic metal concentrations[110] Only occasional spontaneous cases of ICT arise today.
Cancer
Cancer is a complicated disease that is not well understood. Some researchers are investigating the possible role of copper in angiogenesis associated with different types of cancers.[111] A copper chelator, tetrathiomolybdate, which depletes copper stores in the body, is under investigation as an anti-angiogenic agent in pilot[112] and clinical trials.[113] The drug may inhibit tumor angiogenesis in hepatocellular carcinoma, pleural mesothelioma, colorectal cancer, head and neck squamos cell carcinoma, breast cancer, and kidney cancer.[114] The copper complex of a synthetic salicylaldehyde pyrazole hydrazone (SPH) derivative induced human umbilical endothelial cell (HUVEC) apoptosis and showed anti-angiogenesis effect in vitro.[115]
The trace element copper had been found promoting tumor growth.[116][117] Several evidence from animal models indicates that tumors concentrate high levels of copper. Meanwhile, extra copper has been found in some human cancers.[118][119] Recently, therapeutic strategies targeting copper in the tumor have been proposed. Upon administration with a specific copper chelator, copper complexes would be formed at a relatively high level in tumors. Copper complexes are often toxic to cells, therefore tumor cells were killed, while normal cells in the whole body remained alive for the lower level of copper.[120]
Some copper chelators get more effective or novel bioactivity after forming copper-chelator complexes. It was found that Cu2+ was critically needed for PDTC induced apoptosis in HL-60 cells.[121] The copper complex of salicylaldehyde benzoylhydrazone (SBH) derivatives showed increased efficacy of growth inhibition in several cancer cell lines, when compared with the metal-free SBHs.[122][123][124]
SBHs can react with many kinds of transition metal cations and thereby forming a number of complexes.[124][125][126] Copper-SBH complexes were more cytotoxic than complexes of other transitional metals (Cu > Ni > Zn = Mn > Fe = Cr > Co) in MOLT-4 cells, an established human T-cell leukemia cell line. SBHs, especially their copper complexes appeared to be potent inhibitors of DNA synthesis and cell growth in several human cancer cell lines, and rodent cancer cell lines.[122][123]
Salicylaldehyde pyrazole hydrazone (SPH) derivatives were found to inhibit the growth of A549 lung carcinoma cells.[127] SPH has identical ligands for Cu2+ as SBH. The Cu-SPH complex was found to induce apoptosis in A549, H322 and H1299 lung cancer cells.[128]
Contraception with copper IUDs
Main articles: IUD with copper and Paragard
A copper intrauterine device (IUD) is a type of long-acting reversible contraception that is considered to be one of the most effective forms of birth control.[129] It is also considered the most effective non-hormonal contraceptive device. The copper IUD's primary mechanism of action is to prevent fertilization. Active substances released from the IUD, together with products derived from the inflammatory reaction present in the luminal fluids of the genital tract, are toxic for spermatozoa and oocytes, preventing the encounter of healthy gametes and the formation of viable embryos.
Plant and animal health
In addition to being an essential nutrient for humans, copper is vital for the health of animals and plants and plays an important role in agriculture.[130]
Plant health
Copper concentrations in soil are not uniform around the world. In many areas, soils have insufficient levels of copper. Soils that are naturally deficient in copper often require copper supplements before agricultural crops, such as cereals, can be grown.
Copper deficiencies in soil can lead to crop failure. Copper deficiency is a major issue in global food production, resulting in losses in yield and reduced quality of output. Nitrogen fertilizers can worsen copper deficiency in agricultural soils.
The world's two most important food crops, rice and wheat, are highly susceptible to copper deficiency. So are several other important foods, including citrus, oats, spinach and carrots. On the other hand, some foods including coconuts, soybeans and asparagus, are not particularly sensitive to copper-deficient soils.
The most effective strategy to counter copper deficiency is to supplement the soil with copper, usually in the form of copper sulfate. Sewage sludge is also used in some areas to replenish agricultural land with organics and trace metals, including copper.
Animal health
In livestock, cattle and sheep commonly show indications when they are copper deficient. Swayback, a sheep disease associated with copper deficiency, imposes enormous costs on farmers worldwide, particularly in Europe, North America, and many tropical countries. For pigs, copper has been shown to be an outstanding growth promoter.
See also
References
- 1 2 Scheiber, Ivo; Dringen, Ralf; Mercer, Julian F. B. (2013). "Copper: Effects of Deficiency and Overload". In Sigel, Astrid; Sigel, Helmut; Sigel, Roland K.O. Interrelations between Essential Metal Ions and Human Diseases. Metal Ions in Life Sciences. 13. Springer. pp. 359–87. doi:10.1007/978-94-007-7500-8_11. ISBN 978-94-007-7500-8.
- ↑ Hart, E. B.; Steenbock, H.; Waddell, J. (1928). "Iron nutrition. VII: Copper is a supplement to iron for hemoglobin building in the rat". The Journal of Biological Chemistry. 77: 797–833.
- 1 2 3 4 5 6 Ralph, A., and McArdle, H. J. 2001. Copper metabolism and requirements in the pregnant mother, her fetus, and children. New York: International Copper Association
- ↑ George Obikoya, http://vitamins-nutrition.org/vitamins/copper.html
- ↑ http://copperinfo.com/health/pregnancy.html.
- ↑ Vest, Katherine E.; Hashemi, Hayaa F.; Cobine, Paul A. (2013). "The Copper Metallome in Eukaryotic Cells". In Banci, Lucia. Metallomics and the Cell. Metal Ions in Life Sciences. 12. Springer. doi:10.1007/978-94-007-5561-10_12. ISBN 978-94-007-5560-4.
- 1 2 3 4 5 6 Stern, Bonnie Ransom; Solioz, Marc; Krewski, Daniel; Aggett, Peter; Aw, Tar-Ching; Baker, Scott; Crump, Kenny; Dourson, Michael; Haber, Lynne; Hertzberg, Rick; Keen, Carl; Meek, Bette; Rudenko, Larisa; Schoeny, Rita; Slob, Wout; Starr, Tom (2007). "Copper and Human Health: Biochemistry, Genetics, and Strategies for Modeling Dose-response Relationships". Journal of Toxicology and Environmental Health, Part B. 10 (3): 157–222. doi:10.1080/10937400600755911. PMID 17454552.
- 1 2 3 4 5 6 7 8 Stern, Bonnie Ransom (2010). "Essentiality and Toxicity in Copper Health Risk Assessment: Overview, Update and Regulatory Considerations". Journal of Toxicology and Environmental Health, Part A. 73 (2): 114–27. doi:10.1080/15287390903337100. PMID 20077283.
- 1 2 3 4 5 6 7 8 9 10 11 International Programme on Chemical Safety. 1998. Environmental Health Criteria No. 200: Copper. Geneva: World Health Organization
- 1 2 Camakaris, J.; Voskoboinik, I.; Mercer, J.F. (1999). "Molecular Mechanisms of Copper Homeostasis". Biochemical and Biophysical Research Communications. 261 (2): 225–32. doi:10.1006/bbrc.1999.1073. PMID 10425169.
- 1 2 3 Harris, Edward D. (2000). "Cellular copper transport and metabolism". Annual Review of Nutrition. 20 (1): 291–310. doi:10.1146/annurev.nutr.20.1.291. PMID 10940336.
- 1 2 Harris, Edward D. (2001). "Copper Homeostasis: The Role of Cellular Transporters". Nutrition Reviews. 59 (9): 281–5. doi:10.1111/j.1753-4887.2001.tb07017.x. PMID 11570430.
- ↑ Bertinato, Jesse; L'Abbé, Mary R. (2004). "Maintaining copper homeostasis: regulation of copper-trafficking proteins in response to copper deficiency or overload". The Journal of Nutritional Biochemistry. 15 (6): 316–22. doi:10.1016/j.jnutbio.2004.02.004. PMID 15157936.
- ↑ Lewis, Al, 2009, The Hygienic Benefits of Antimicrobial Copper Alloy Surfaces In Healthcare Settings, a compilation of information and data for the International Copper Association Inc., © 2009, available from International Copper Association Inc., A1335-XX/09
- ↑ Stern, B.R. et. al, 2007, Copper And Human Health: Biochemistry, Genetics, And Strategies for Modeling Dose-Response Relationships, Journal of Toxicology and Environmental Health, Part B, 10:157–222
- ↑ van Campen, Darrell R.; Mitchell, Elizabeth A. (1965). "Absorption of Cu64, Zn65, Mo99, and Fe59 from ligated segments of the rat gastrointestinal tract". The Journal of Nutrition. 86 (2): 120–4. PMID 14302118.
- ↑ Crampton, R. F.; Matthews, D. M.; Poisner, Roselle (1965). "Observations on the mechanism of absorption of copper by the small intestine". The Journal of Physiology. 178 (1): 111–26. doi:10.1113/jphysiol.1965.sp007618. PMC 1357280
 . PMID 14298103.
. PMID 14298103. - ↑ Bearn, AG; Kunkel, HG (1955). "Metabolic studies in Wilson's disease using Cu64". The Journal of Laboratory and Clinical Medicine. 45 (4): 623–31. PMID 14368026.
- ↑ Strickland, GT; Beckner, WM; Leu, ML (1972). "Absorption of copper in homozygotes and heterozygotes for Wilson's disease and controls: isotope tracer studies with 67 Cu and 64 Cu". Clinical Science. 43 (5): 617–25. doi:10.1042/cs0430617. PMID 5083937.
- ↑ Strickland, GT; Beckner, WM; Leu, ML; O'Reilly, S (1972). "Turnover studies of copper in homozygotes and heterozygotes for Wilson's disease and controls: isotope tracer studies with 67 Cu". Clinical Science. 43 (5): 605–15. doi:10.1042/cs0430605. PMID 5083936.
- ↑ Turnlund, Judith R; Keyes, William R; Anderson, Helen L; Acord, Lorra L (1989). "Copper absorption and retention in young men at three levels of dietary copper by use of the stable isotope 65Cu1–4". The American Journal of Clinical Nutrition. 49 (5): 870–8. PMID 2718922.
- ↑ Turnlund, Judith R. (1998). "Human whole-body copper metabolism". The American Journal of Clinical Nutrition. 67 (5 Suppl): 960S–964S. PMID 9587136.
- ↑ Ehrenkranz, Richard A.; Gettner, Patricia A.; Nelli, Catherine M. (1989). "Nutrient Balance Studies in Premature Infants Fed Premature Formula or Fortified Preterm Human Milk". Journal of Pediatric Gastroenterology and Nutrition. 8 (1): 58–67. doi:10.1097/00005176-198901000-00012. PMID 2499673.
- ↑ World Health Organization. 1998, Guidelines for drinking-water quality. Addendum to Volume 2, 2nd ed. Geneva
- ↑ Turnlund, Judith R; Swanson, Christine A; King, Janet C (1983). "Copper Absorption and Retention in Pregnant Women Fed Diets Based on Animal and Plant Proteins". The Journal of Nutrition. 113 (11): 2346–52. PMID 6631551.
- ↑ Cousins, Robert J (1985). "Absorption, transport, and hepatic metabolism of copper and zinc: special reference to metallothionein and ceruloplasmin". Physiological Reviews. 65 (2): 238–309. PMID 3885271.
- ↑ Oestreicher, Paul; Cousins, Robert J (1985). "Copper and Zinc Absorption in the Rat: Mechanism of Mutual Antagonism". The Journal of Nutrition. 115 (2): 159–66. PMID 3968585.
- 1 2 Lee, D; Schroeder, J; Gordon, DT (January 1984). "The effect of phytic acid on copper bioavailability". Federation Proceedings. Federation of American Societies for Experimental Biology. 43 (3): 616–20.
- ↑ Greger, JL; Mulvaney, Jude (1985). "Absorption and Tissue Distribution of Zinc, Iron and Copper by Rats Fed Diets Containing Lactalbumin, Soy and Supplemental Sulfur-Containing Amino Acids". The Journal of Nutrition. 115 (2): 200–10. PMID 4038512.
- ↑ Werman, Moshe J.; Bhathena, Sam J. (1995). "Fructose metabolizing enzymes in the rat liver and metabolic parameters: Interactions between dietary copper, type of carbohydrates, and gender". The Journal of Nutritional Biochemistry. 6 (7): 373–379. doi:10.1016/0955-2863(95)80005-W. PMID 12049998.
- 1 2 Wapnir, Raul A (1998). "Copper absorption and bioavailability". The American Journal of Clinical Nutrition. 67 (5 Suppl): 1054S–1060S. PMID 9587151.
- 1 2 3 "Archived copy". Archived from the original on 2010-10-15. Retrieved 2010-10-20. [https://web.archive.org/web/20101015204256/http://www.copperinfo.com:80/health/goodhealth.html "Archived copy". Archived from the original on 2010-10-15. Retrieved 2010-10-20. Archived] October 15, 2010, at the Wayback Machine.
- ↑ Lutsenko, Svetlana; Kaplan, Jack H. (1995). "Organization of P-type ATPases: significance of structural diversity". Biochemistry. 34 (48): 15607–13. doi:10.1021/bi00048a001. PMID 7495787.
- ↑ Solioz, Marc; Vulpe, Christopher (1996). "CPx-type ATPases: a class of P-type ATPases that pump heavy metals". Trends in Biochemical Sciences. 21 (7): 237–41. doi:10.1016/S0968-0004(96)20016-7. PMID 8755241.
- ↑ Lee, J.; Petris, M. J.; Thiele, D. J. (2002). "Characterization of mouse embryonic cells deficient in the ctr1 high affinity copper transporter: Identification of a Ctr1-independent copper transport system". The Journal of Biological Chemistry. 277 (43): 40253–9. doi:10.1074/jbc.M208002200. PMID 12177073.
- ↑ Marceau, N; Aspin, N; Sass-Kortsak, A (1970). "Absorption of copper 64 from gastrointestinal tract of the rat". The American Journal of Physiology. 218 (2): 377–83. PMID 5412451.
- ↑ Bligh, S.W.Annie; Boyle, Helena A.; Mcewen, Andrew B.; Sadler, Peter J.; Woodham, Robert H. (1992). "1H NMR studies of reactions of copper complexes with human blood plasma and urine". Biochemical Pharmacology. 43 (2): 137–45. doi:10.1016/0006-2952(92)90270-S. PMID 1739401.
- ↑ Linder, Maria C; Hazegh-Azam, Maryam (1996). "Copper biochemistry and molecular biology". The American Journal of Clinical Nutrition. 63 (5): 797S–811S. PMID 8615367.
- ↑ Linder, Maria C; Wooten, Lisa; Cerveza, Philip; Cotton, Steven; Shulze, Roman; Lomeli, Norma (1998). "Copper transport". The American Journal of Clinical Nutrition. 67 (5 Suppl): 965S–971S. PMID 9587137.
- ↑ Cousins, RJ (1985). "Absorption, transport, and hepatic metabolism of copper and zinc: special reference to metallothionein and ceruloplasmin". Physiological Reviews. 65 (2): 238–309. PMID 3885271.
- ↑ Winge, Dennis R.; Mehra, Rajesh K. (1990). "Host Defenses against Copper Toxicity". International Review of Experimental Pathology. 31: 47–83. doi:10.1016/b978-0-12-364931-7.50007-0. PMID 2292474.
- ↑ Turnlund, Judith R (1998). "Human whole-body copper metabolism". The American Journal of Clinical Nutrition. 67 (5 Suppl): 960S–964S. PMID 9587136.
- ↑ Aggett, PJ (1999). "An overview of the metabolism of copper". European Journal of Medical Research. 4 (6): 214–6. PMID 10383873.
- ↑ WHO/FAO/IAEA, (1996), Trace Elements in Human Nutrition and Health. World Health Organization, Geneva)
- 1 2 MedlinePlus Encyclopedia Copper in diet
- 1 2 3 "Copper". Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. National Academies Press. 2001. pp. 224–57. ISBN 978-0-309-07279-3.
- 1 2 Trumbo, Paula; Yates, Allison A; Schlicker, Sandra; Poos, Mary (2001). "Dietary Reference Intakes". Journal of the American Dietetic Association. 101 (3): 294–301. doi:10.1016/S0002-8223(01)00078-5. PMID 11269606.
- ↑ Georgopoulos, PG; Roy, A; Yonone-Lioy, MJ; Opiekun, RE; Lioy, PJ (2001). "Environmental copper: its dynamics and human exposure issues". Journal of Toxicology and Environmental Health. Part B, Critical Reviews. 4 (4): 341–94. doi:10.1080/109374001753146207. PMID 11695043.
- 1 2 Sadhra, Steven S.; Wheatley, Andrew D.; Cross, Hilary J. (2007). "Dietary exposure to copper in the European Union and its assessment for EU regulatory risk assessment". Science of The Total Environment. 374 (2-3): 223–34. doi:10.1016/j.scitotenv.2006.12.041. PMID 17270248.
- ↑ World Health Organization. 1998. Copper. Environmental Health Criteria 200. Geneva: IPCS, WHO
- 1 2 3 4 5 6 7 8 9 Stern, Bonnie Ransom (2007). "U-Shaped Dose-Response Curve for Risk Assessment of Essential Trace Elements: Copper as a Case Study". In Robson, Mark G.; Toscano, William A. Risk Assessment for Environmental Health. San Francisco: John Wiley and Sons. pp. 555–62. ISBN 978-1-118-42406-3.
- 1 2 http://copperinfo.com/health/facts.html
- ↑ Georgopoulos, Panos G; Wang, Sheng Wei; Georgopoulos, Ioannis G; Yonone-Lioy, Mary Jean; Lioy, Paul J (2006). "Assessment of human exposure to copper: A case study using the NHEXAS database". Journal of Exposure Analysis and Environmental Epidemiology. 16 (5): 397–409. doi:10.1038/sj.jea.7500462. PMID 16249795.
- ↑ Spinazzi, Marco; De Lazzari, Franca; Tavolato, Bruno; Angelini, Corrado; Manara, Renzo; Armani, Mario (2007). "Myelo-optico-neuropathy in copper deficiency occurring after partial gastrectomy". Journal of Neurology. 254 (8): 1012–7. doi:10.1007/s00415-006-0479-2. PMID 17415508.
- ↑ Goodman, B P; Bosch, E P; Ross, M A; Hoffman-Snyder, C; Dodick, D D; Smith, B E (2009). "Clinical and electrodiagnostic findings in copper deficiency myeloneuropathy". Journal of Neurology, Neurosurgery & Psychiatry. 80 (5): 524–7. doi:10.1136/jnnp.2008.144683. PMID 18495738.
- ↑ Kumar, Neeraj; Elliott, Michelle A.; Hoyer, James D.; Harper, Charles M.; Ahlskog, J. Eric; Phyliky, Robert L. (2005). "'Myelodysplasia,' Myeloneuropathy, and Copper Deficiency". Mayo Clinic Proceedings. 80 (7): 943–6. doi:10.4065/80.7.943. PMID 16007901.
- ↑ Cordano, A (1978). "Copper deficiency in clinical medicine". In Hambidge, K. M.; Nichols, B. L. Zinc and Copper in Clinical Medicine. New York: SP Med. Sci. Books. pp. 119–26.
- 1 2 Danks, D M (1988). "Copper Deficiency in Humans". Annual Review of Nutrition. 8: 235–57. doi:10.1146/annurev.nu.08.070188.001315. PMID 3060166.
- ↑ Klevay, LM (1980). "The influence of copper and zinc on the occurrence of ischemic heart disease". Journal of Environmental Pathology and Toxicology. 4 (2-3): 281–7. PMID 7007558.
- ↑ Strain, J. J. (1994). "Newer aspects of micronutrients in chronic disease: copper". Proceedings of the Nutrition Society. 53 (3): 583–98. doi:10.1079/PNS19940067. PMID 7886057.
- ↑ Salem, Harry; Green, Sidney; Bigelow, Sanford; Borzelleca, Joseph; Baskin, Steven (1992). "Preface". Critical Reviews in Food Science and Nutrition. 32 (1): 1–31. doi:10.1080/10408399209527583. PMID 1290583.
- ↑ Kaegi, Jeremias H. R.; Schaeffer, Andreas (1988). "Biochemistry of metallothionein". Biochemistry. 27 (23): 8509–15. doi:10.1021/bi00423a001. PMID 3064814.
- ↑ Lönnerdal, Bo (1996). "Bioavailability of copper". The American Journal of Clinical Nutrition. 63 (5): 821S–9S. PMID 8615369.
- ↑ Kelsay, JL (1987). "Effects of fiber, phytic acid, and oxalic acid in the diet on mineral bioavailability". The American Journal of Gastroenterology. 82 (10): 983–6. PMID 2821800.
- 1 2 3 U.S. National Research Council. 2000. Copper in drinking water. Committee on Copper in Drinking Water, Board on Environmental Studies and Toxicology, Commission of Life Sciences. Washington, DC: National Academy Press
- ↑ Bremner, Ian (1998). "Manifestations of copper excess". The American Journal of Clinical Nutrition. 67 (5 Suppl): 1069S–1073S. PMID 9587154.
- ↑ Bartzokis, George; Sultzer, David; Cummings, Jeffrey; Holt, Lori E.; Hance, Darwood B.; Henderson, Victor W.; Mintz, Jim (2000). "In Vivo Evaluation of Brain Iron in Alzheimer Disease Using Magnetic Resonance Imaging". Archives of General Psychiatry. 57 (1): 47–53. doi:10.1001/archpsyc.57.1.47. PMID 10632232. Lay summary – WebMD Health News (February 28, 1000).
- ↑ Duce, James A.; Tsatsanis, Andrew; Cater, Michael A.; James, Simon A.; Robb, Elysia; Wikhe, Krutika; Leong, Su Ling; Perez, Keyla; Johanssen, Timothy; Greenough, Mark A.; Cho, Hyun-Hee; Galatis, Denise; Moir, Robert D.; Masters, Colin L.; McLean, Catriona; Tanzi, Rudolph E.; Cappai, Roberto; Barnham, Kevin J.; Ciccotosto, Giuseppe D.; Rogers, Jack T.; Bush, Ashley I. (2010). "Iron-Export Ferroxidase Activity of β-Amyloid Precursor Protein Is Inhibited by Zinc in Alzheimer's Disease". Cell. 142 (6): 857–67. doi:10.1016/j.cell.2010.08.014. PMC 2943017. PMID 20817278. Lay summary – New Scientist (September 8, 2010).
- ↑ "Am I at risk of developing dementia?". Alzheimer's Society.
- ↑ Brewer, George J. (2010). "Copper toxicity in the general population". Clinical Neurophysiology. 121 (4): 459–60. doi:10.1016/j.clinph.2009.12.015. PMID 20071223.
- 1 2 3 4 Llanos, Roxana M.; Mercer, Julian F.B. (2002). "The Molecular Basis of Copper Homeostasis Copper-Related Disorders". DNA and Cell Biology. 21 (4): 259–70. doi:10.1089/104454902753759681. PMID 12042066.
- ↑ Copper link to Alzheimer's disease, New Scientist, August 12, 2003, http://www.newscientist.com/article/dn4045-copper-link-to-alzheimers-disease.html
- ↑ Singh, Itender; Sagare, Abhay P.; Coma, Mireia; Perlmutter, David; Gelein, Robert; Bell, Robert D.; Deane, Richard J.; Zhong, Elaine; Parisi, Margaret; Ciszewski, Joseph; Kasper, R. Tristan; Deane, Rashid (2013). "Low levels of copper disrupt brain amyloid-β homeostasis by altering its production and clearance". Proceedings of the National Academy of Sciences. 110 (36): 14771–6. Bibcode:2013PNAS..11014771S. doi:10.1073/pnas.1302212110. PMC 3767519. PMID 23959870. Lay summary – ScienceDaily (November 8, 2007).
- ↑ Loef, Martin; Walach, Harald (2012-01-01). "Copper and iron in Alzheimer's disease: a systematic review and its dietary implications". The British Journal of Nutrition. 107 (1): 7–19. doi:10.1017/S000711451100376X. ISSN 1475-2662. PMID 21767446.
- ↑ Protective role for copper in Alzheimer's disease, Science News, October 13, 2009, http://www.sciencedaily.com/releases/2009/10/091008133457.htm
- ↑ Kaden, Daniela; Bush, Ashley I.; Danzeisen, Ruth; Bayer, Thomas A.; Multhaup, Gerd (2011). "Disturbed Copper Bioavailability in Alzheimer's Disease". International Journal of Alzheimer's Disease. 2011: 345614. doi:10.4061/2011/345614. PMC 3227474. PMID 22145082.
- ↑ Kessler, Holger; Bayer, Thomas A.; Bach, Daniela; Schneider-Axmann, Thomas; Supprian, Tillmann; Herrmann, Wolfgang; Haber, Manfred; Multhaup, Gerd; Falkai, Peter; Pajonk, Frank-Gerald (2008). "Intake of copper has no effect on cognition in patients with mild Alzheimer's disease: a pilot phase 2 clinical trial". Journal of Neural Transmission. 115 (8): 1181–7. doi:10.1007/s00702-008-0080-1. PMC 2516533. PMID 18587525.
- ↑ Kessler, Holger; Pajonk, Frank-Gerald; Bach, Daniela; Schneider-Axmann, Thomas; Falkai, Peter; Herrmann, Wolfgang; Multhaup, Gerd; Wiltfang, Jens; Schäfer, Stephanie; Wirths, Oliver; Bayer, Thomas A. (2008). "Effect of copper intake on CSF parameters in patients with mild Alzheimer's disease: a pilot phase 2 clinical trial". Journal of Neural Transmission. 115 (12): 1651–9. doi:10.1007/s00702-008-0136-2. PMID 18972062.
- ↑ Brewer, George J. (2012). "Copper toxicity in Alzheimer's disease: Cognitive loss from ingestion of inorganic copper". Journal of Trace Elements in Medicine and Biology. 26 (2-3): 89–92. doi:10.1016/j.jtemb.2012.04.019. PMID 22673823.
- ↑ Brewer, George J. (2000). "Editorial: Is heterozygosity for a Wilson's disease gene defect an important underlying cause of infantile and childhood copper toxicosis syndromes?". The Journal of Trace Elements in Experimental Medicine. 13 (3): 249–54. doi:10.1002/1520-670X(2000)13:3<249::AID-JTRA1>3.0.CO;2-L.
- ↑ Araya, Magdalena; McGoldrick, Marie Clare; Klevay, Leslie M.; Strain, J.J.; Robson, Paula; Nielsen, Forrest; Olivares, Manuel; Pizarro, Fernando; Johnson, LuAnn; Poirier, Kenneth A. (2001). "Determination of an Acute No-Observed-Adverse-Effect Level (NOAEL) for Copper in Water". Regulatory Toxicology and Pharmacology. 34 (2): 137–45. doi:10.1006/rtph.2001.1492. PMID 11603956.
- ↑ Araya, Magdalena; Chen, Bingheng; Klevay, Leslie M; Strain, J.J; Johnson, LuAnn; Robson, Paula; Shi, Wei; Nielsen, Forrest; Zhu, Huigang; Olivares, Manuel; Pizarro, Fernando; Haber, Lynne T (2003). "Confirmation of an acute no-observed-adverse-effect and low-observed-adverse-effect level for copper in bottled drinking water in a multi-site international study". Regulatory Toxicology and Pharmacology. 38 (3): 389–99. doi:10.1016/j.yrtph.2003.08.001. PMID 14623488.
- ↑ Pizarro, F.; Olivares, M.; Gidi, V.; Araya, M. (1999). "The Gastrointestinal Tract and Acute Effects of Copper in Drinking Water and Beverages". Reviews on Environmental Health. 14 (4): 231–8. doi:10.1515/REVEH.1999.14.4.231. PMID 10746735.
- ↑ Pizarro, F; Olivares, M; Uauy, R; Contreras, P; Rebelo, A; Gidi, V (1999). "Acute gastrointestinal effects of graded levels of copper in drinking water". Environmental Health Perspectives. 107 (2): 117–21. doi:10.1289/ehp.99107117. PMC 1566323. PMID 9924006.
- ↑ Zacarías, I; Yáñez, CG; Araya, M; Oraka, C; Olivares, M; Uauy, R (2001). "Determination of the taste threshold of copper in water". Chemical Senses. 26 (1): 85–9. doi:10.1093/chemse/26.1.85. PMID 11124219.
- ↑ Olivares, Manuel; Uauy, Ricardo (1996). "Limits of metabolic tolerance to copper and biological basis for present recommendations and regulations". The American Journal of Clinical Nutrition. 63 (5): 846S–52S. PMID 8615373.
- ↑ O'Donohue, J; Reid, M; Varghese, A; Portmann, B; Williams, R (1999). "A case of adult chronic copper self-intoxication resulting in cirrhosis". European Journal of Medical Research. 4 (6): 252. PMID 10383882.
- ↑ Buchanan, Sharunda D.; Diseker, Robert A.; Sinks, Thomas; Olson, David R.; Daniel, Jack; Flodman, Thomas (1999). "Copper in Drinking Water, Nebraska, 1994". International Journal of Occupational and Environmental Health. 5 (4): 256–61. doi:10.1179/oeh.1999.5.4.256. PMID 10633241.
- ↑ Araya, Magdalena; Olivares, Manuel; Pizarro, Fernando; González, Mauricio; Speisky, Hernán; Uauy, Ricardo (2003). "Gastrointestinal symptoms and blood indicators of copper load in apparently healthy adults undergoing controlled copper exposure". The American Journal of Clinical Nutrition. 77 (3): 646–50. PMID 12600855.
- ↑ O’Connor, J.M.; Bonham, M.P.; Turley, E.; McKeown, A.; McKelvey-Martin, V.J.; Gilmore, W.S.; Strain, J.J. (2003). "Copper Supplementation Has No Effect on Markers of DNA Damage and Liver Function in Healthy Adults (FOODCUE Project)". Annals of Nutrition and Metabolism. 47 (5): 201–6. doi:10.1159/000070486. PMID 12748413.
- ↑ Pratt, William B; Omdahl, John L; Sorenson, John RJ (1985). "Lack of effects of copper gluconate supplementation". The American Journal of Clinical Nutrition. 42 (4): 681–2. PMID 2931973.
- ↑ Turley, Eithne; McKeown, Andrea; Bonham, Maxine P.; O’Connor, Jacqueline M.; Chopra, Mridula; Harvey, Linda J.; Majsak-Newman, Gosia; Fairweather-Tait, Susan J.; Bügel, Susanne; Sandström, Brittmarie; Rock, Edmond; Mazur, Andrzej; Rayssiguier, Yves; Strain, J.J. (2000). "Copper supplementation in humans does not affect the susceptibility of low density lipoprotein to in vitro induced oxidation (FOODCUE project)". Free Radical Biology and Medicine. 29 (11): 1129–34. doi:10.1016/S0891-5849(00)00409-3. PMID 11121720.
- ↑ Olivares, Manuel; Pizarro, Fernando; Speisky, Hernán; Lönnerdal, Bo; Uauy, Ricardo (1998). "Copper in Infant Nutrition: Safety of World Health Organization Provisional Guideline Value for Copper Content of Drinking Water". Journal of Pediatric Gastroenterology & Nutrition. 26 (3): 251–7. doi:10.1097/00005176-199803000-00003. PMID 9523857.
- ↑ Milne, David B (1998). "Copper intake and assessment of copper status". The American Journal of Clinical Nutrition. 67 (5 Suppl): 1041S–1045S. PMID 9587149.
- ↑ http://copperinfo.com/health/goodhealth.hereditary.html[]
- 1 2 3 4 Kaler, Stephen G. (1998). "Metabolic and molecular bases of Menkes disease and occipital horn syndrome". Pediatric and Developmental Pathology. 1 (1): 85–98. doi:10.1007/s100249900011. PMID 10463276.
- 1 2 Kaler, Stephen G. (1996). "Menkes disease mutations and response to early copper histidine treatment". Nature Genetics. 13 (1): 21–2. doi:10.1038/ng0596-21. PMID 8673098.
- ↑ Kaler, SG (1994). "Menkes disease". Advances in Pediatrics. 41: 263–304. PMID 7992686.
- 1 2 http://copperinfo.com/health/goodhealth.genetic.html[]
- ↑ Mercer, Julian F B (2001). "The molecular basis of copper-transport diseases". Trends in Molecular Medicine. 7 (2): 64–9. doi:10.1016/S1471-4914(01)01920-7. PMID 11286757.
- ↑ Gitlin, Jonathan D (2003). "Wilson disease". Gastroenterology. 125 (6): 1868–77. doi:10.1053/j.gastro.2003.05.010. PMID 14724838.
- ↑ Scheinberg, I Herbert; Sternlieb, Irmin (1996). "Wilson disease and idiopathic copper toxicosis". The American Journal of Clinical Nutrition. 63 (5): 842S–5S. PMID 8615372.
- 1 2 Ferenci, Peter; Caca, Karel; Loudianos, Georgios; Mieli-Vergani, Georgina; Tanner, Stuart; Sternlieb, Irmin; Schilsky, Michael; Cox, Diane; Berr, Frieder (2003). "Diagnosis and phenotypic classification of Wilson disease". Liver International. 23 (3): 139–42. doi:10.1034/j.1600-0676.2003.00824.x. PMID 12955875.
- ↑ Brewer, George J.; Dick, Robert D.; Johnson, Virginia D.; Brunberg, James A.; Kluin, Karen J.; Fink, John K. (1998). "Treatment of Wilson's disease with zinc: XV long-term follow-up studies". Journal of Laboratory and Clinical Medicine. 132 (4): 264–78. doi:10.1016/s0022-2143(98)90039-7. PMID 9794697.
- ↑ Brewer, George J.; Johnson, Virginia; Dick, Robert D.; Kluin, Karen J.; Fink, John K.; Brunberg, James A. (1996). "Treatment of Wilson Disease With Ammonium Tetrathiomolybdate". Archives of Neurology. 53 (10): 1017–25. doi:10.1001/archneur.1996.00550100103019. PMID 8859064.
- ↑ Garciavillarreal, L; Daniels, S; Shaw, S; Cotton, D; Galvin, M; Geskes, J; Bauer, P; Sierrahernandez, A; Buckler, A; Tugores, A (2000). "High prevalence of the very rare wilson disease gene mutation Leu708Pro in the Island of Gran Canaria (Canary Islands, Spain): A genetic and clinical study". Hepatology. 32 (6): 1329–36. doi:10.1053/jhep.2000.20152. PMID 11093740.
- ↑ Ha-Hao, Duc; Hefter, Harald; Stremmel, Wolfgang; Castañeda-Guillot, Carlos; Hernández, Ana Hernández; Cox, Diane W; Auburger, Georg (1998). "His1069Gln and six novel Wilson disease mutations: analysis of relevance for early diagnosis and phenotype". European Journal of Human Genetics. 6 (6): 616–23. doi:10.1038/sj.ejhg.5200237. PMID 9887381.
- ↑ Wijmenga, C; Müller, T; Murli, I S; Brunt, T; Feichtinger, H; Schönitzer, D; Houwen, R H J; Müller, W; Sandkuijl, L A; Pearson, P L (1998). "Endemic Tyrolean infantile cirrhosis is not an allelic variant of Wilson's disease". European Journal of Human Genetics. 6 (6): 624–8. doi:10.1038/sj.ejhg.5200235. PMID 9887382.
- 1 2 3 Müller, Thomas; Müller, Wilfried; Feichtinger, Hans (1998). "Idiopathic copper toxicosis". The American Journal of Clinical Nutrition. 67 (5 Suppl): 1082S–1086S. PMID 9587156.
- ↑ Dieter, HH; Schimmelpfennig, W; Meyer, E; Tabert, M (1999). "Early childhood cirrhoses (ECC) in Germany between 1982 and 1994 with special consideration of copper etiology". European Journal of Medical Research. 4 (6): 233–42. PMID 10383878.
- ↑ Goodman, Vicki; Brewer, George; Merajver, Sofia (2005). "Control of Copper Status for Cancer Therapy". Current Cancer Drug Targets. 5 (7): 543–9. doi:10.2174/156800905774574066. PMID 16305350.
- ↑ Gartner, Elaina M.; Griffith, Kent A.; Pan, Quintin; Brewer, George J.; Henja, Gwen F.; Merajver, Sofia D.; Zalupski, Mark M. (2009). "A pilot trial of the anti-angiogenic copper lowering agent tetrathiomolybdate in combination with irinotecan, 5-flurouracil, and leucovorin for metastatic colorectal cancer". Investigational New Drugs. 27 (2): 159–65. doi:10.1007/s10637-008-9165-9. PMC 4171042. PMID 18712502.
- ↑ Pass, Harvey I.; Brewer, George J.; Dick, Robert; Carbone, Michele; Merajver, Sofia (2008). "A Phase II Trial of Tetrathiomolybdate After Surgery for Malignant Mesothelioma: Final Results". The Annals of Thoracic Surgery. 86 (2): 383–9; discussion 390. doi:10.1016/j.athoracsur.2008.03.016. PMID 18640301.
- ↑ Brewer, G. J.; Merajver, S. D. (2002). "Cancer Therapy With Tetrathiomolybdate: Antiangiogenesis by Lowering Body Copper—A Review". Integrative Cancer Therapies. 1 (4): 327–37. doi:10.1177/1534735402238185. PMID 14664727.
- ↑ Fan, Chuandong; Zhao, Jing; Zhao, Baoxiang; Zhang, Shangli; Miao, Junying (2009). "Novel Complex of Copper and a Salicylaldehyde Pyrazole Hydrazone Derivative Induces Apoptosis through Up-Regulating Integrin β4 in Vascular Endothelial Cells". Chemical Research in Toxicology. 22 (9): 1517–25. doi:10.1021/tx900111y. PMID 19621939.
- ↑ Brewer, George J. (2001). "Copper Control as an Antiangiogenic Anticancer Therapy: Lessons from Treating Wilson's Disease". Experimental Biology and Medicine. 226 (7): 665–73. PMID 11444102.
- ↑ Lowndes, Sarah A.; Harris, Adrian L. (2005). "The Role of Copper in Tumour Angiogenesis". Journal of Mammary Gland Biology and Neoplasia. 10 (4): 299–310. doi:10.1007/s10911-006-9003-7. PMID 16924372.
- ↑ Díez, M.; Arroyo, M.; Cerdàn, F.J.; Muñoz, M.; Martin, M.A.; Balibrea, J.L. (1989). "Serum and Tissue Trace Metal Levels in Lung Cancer". Oncology. 46 (4): 230–4. doi:10.1159/000226722. PMID 2740065.
- ↑ Sharma, K; Mittal, DK; Kesarwani, RC; Kamboj, VP; Chowdhery (1994). "Diagnostic and prognostic significance of serum and tissue trace elements in breast malignancy". Indian Journal of Medical Sciences. 48 (10): 227–32. PMID 7829172.
- ↑ Daniel, Kenyon G; Chen, Di; Orlu, Shirley; Cui, Qiuzhi; Miller, Fred R; Dou, Q Ping (2005). "Clioquinol and pyrrolidine dithiocarbamate complex with copper to form proteasome inhibitors and apoptosis inducers in human breast cancer cells". Breast Cancer Research. 7 (6): R897–908. doi:10.1186/bcr1322. PMC 1410741. PMID 16280039.
- ↑ Chen, Jie; Du, Changsheng; Kang, Jiuhong; Wang, Jianmin (2008). "Cu2+ is required for pyrrolidine dithiocarbamate to inhibit histone acetylation and induce human leukemia cell apoptosis". Chemico-Biological Interactions. 171 (1): 26–36. doi:10.1016/j.cbi.2007.09.004. PMID 17961528.
- 1 2 Johnson, David K.; Murphy, Terrance B.; Rose, Norman J.; Goodwin, William H.; Pickart, Loren (1982). "Cytotoxic chelators and chelates 1. Inhibition of DNA synthesis in cultured rodent and human cells by aroylhydrazones and by a copper(II) complex of salicylaldehyde benzoyl hydrazone". Inorganica Chimica Acta. 67: 159–65. doi:10.1016/S0020-1693(00)85058-6.
- 1 2 Pickart, Loren; Goodwin, William H.; Burgua, William; Murphy, Terrance B.; Johnson, David K. (1983). "Inhibition of the growth of cultured cells and an implanted fibrosarcoma by aroylhydrazone analogs of the Gly-His-Lys-Cu (II) complex". Biochemical Pharmacology. 32 (24): 3868–71. doi:10.1016/0006-2952(83)90164-8. PMID 6661260.
- 1 2 Ainscough, Eric W; Brodie, Andrew M; Denny, William A; Finlay, Graeme J; Gothe, Scott A; Ranford, John D (1999). "Cytotoxicity of salicylaldehyde benzoylhydrazone analogs and their transition metal complexes: quantitative structure–activity relationships". Journal of Inorganic Biochemistry. 77 (3-4): 125–33. doi:10.1016/S0162-0134(99)00131-2. PMID 10643654.
- ↑ Lu, Yi-Heng; Lu, Yu-Wei; Wu, Cheng-Li; Shao, Qun; Chen, Xiao-Ling; Bimbong, Rosa Ngo Biboum (2006). "UV–visible spectroscopic study of the salicyladehyde benzoylhydrazone and its cobalt complexes". Spectrochimica Acta Part A: Molecular and Biomolecular Spectroscopy. 65 (3-4): 695–701. Bibcode:2006AcSpA..65..695L. doi:10.1016/j.saa.2005.12.032. PMID 16503413.
- ↑ Koh, L.L; Kon, O.L; Loh, K.W; Long, Y.C; Ranford, J.D; Tan, A.L.C; Tjan, Y.Y (1998). "Complexes of salicylaldehyde acylhydrazones: Cytotoxicity, QSAR and crystal structure of the sterically hindered t-butyl dimer". Journal of Inorganic Biochemistry. 72 (3-4): 155–62. doi:10.1016/S0162-0134(98)10075-2. PMID 10094614.
- ↑ Xia, Yong; Fan, Chuan-Dong; Zhao, Bao-Xiang; Zhao, Jing; Shin, Dong-Soo; Miao, Jun-Ying (2008). "Synthesis and structure–activity relationships of novel 1-arylmethyl-3-aryl-1H-pyrazole-5-carbohydrazide hydrazone derivatives as potential agents against A549 lung cancer cells". European Journal of Medicinal Chemistry. 43 (11): 2347–53. doi:10.1016/j.ejmech.2008.01.021. PMID 18313806.
- ↑ Fan, ChuanDong; Su, Hua; Zhao, Jing; Zhao, BaoXiang; Zhang, ShangLi; Miao, JunYing (2010). "A novel copper complex of salicylaldehyde pyrazole hydrazone induces apoptosis through up-regulating integrin β4 in H322 lung carcinoma cells". European Journal of Medicinal Chemistry. 45 (4): 1438–46. doi:10.1016/j.ejmech.2009.12.048. PMID 20089331.
- ↑ Winner, Brooke; Peipert, Jeffrey F.; Zhao, Qiuhong; Buckel, Christina; Madden, Tessa; Allsworth, Jenifer E.; Secura, Gina M. (2012). "Effectiveness of Long-Acting Reversible Contraception". New England Journal of Medicine. 366 (21): 1998–2007. doi:10.1056/NEJMoa1110855. PMID 22621627.
- ↑ http://copperinfo.com/health/plant.html[]