Virchow's node
| Virchow's node | |
|---|---|
 Regional lymph tissue. (Supraclavicular near top, in green.)⋅ | |
 Deep Lymph Nodes 1. Submental 2. Submandibular (Submaxillary) Anterior Cervical Lymph Nodes (Deep) 3. Prelaryngeal 4. Thyroid 5. Pretracheal 6. Paratracheal Deep Cervical Lymph Nodes 7. Lateral jugular 8. Anterior jugular 9. Jugulodigastric Inferior Deep Cervical Lymph Nodes 10. Juguloomohyoid 11. Supraclavicular (scalene) | |
Virchow's node (or signal node) is a lymph node in the left supraclavicular fossa (the area above the left clavicle). It takes its supply from lymph vessels in the abdominal cavity. The finding of an enlarged, hard node (also referred to as Troisier's sign) has long been regarded as strongly indicative of the presence of cancer in the abdomen, specifically gastric cancer, that has spread through the lymph vessels. It is sometimes called the signal node or sentinel node for the same reason. Despite this, the concept is not directly related to the sentinel node procedure sometimes used in cancer surgery, and it is also unrelated to the "sentinel gland" of the greater omentum.
It is named after Rudolf Virchow (1821–1902), the German pathologist who first described the gland and its association with gastric cancer in 1848.[1] The French pathologist Charles Emile Troisier noted in 1889 that other abdominal cancers, too, could spread to the node.[2]
Clinical significance
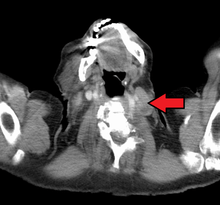
Malignancies of the internal organs can reach an advanced stage before giving symptoms. Stomach cancer, for example, can remain asymptomatic while metastasizing. One of the first visible spots where these tumors metastasize is the left supraclavicular lymph node.
The left supraclavicular node is the classical Virchow's node because it is on the left side of the neck where the lymphatic drainage of most of the body (from the thoracic duct) enters the venous circulation via the left subclavian vein.The metastasis blocks the thoracic duct leading to regurgitation into the surrounding nodes i.e. virchow's node. Another concept is that one of the supraclavicular nodes corresponds to the end node along the thoracic duct and hence the enlargement.[3]
Differential diagnosis of an enlarged Virchow's node includes lymphoma, various intra-abdominal malignancies, breast cancer, and infection (e.g. of the arm). Similarly, an enlarged right supraclavicular lymph node tends to drain thoracic malignancies such as lung and esophageal cancer, as well as Hodgkin's lymphoma.
Additional images
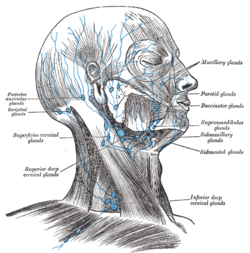 Superficial lymph glands and lymphatic vessels of head and neck.
Superficial lymph glands and lymphatic vessels of head and neck.
References
- ↑ Virchow R (1848). "Zur Diagnose der Krebse in Unterleibe". Med. Reform. 45: 248.
- ↑ Troisier CE (1889). "L'adénopathie sus-claviculaire dans les cancers de l'abdomen". Arch. Gen. Med. 1: 129–138 and 297–309.
- ↑ Mizutani, Masaomi; Nawata, Shin-Ichi; Hirai, Ichiro; Murakami, Gen; Kimura, Wataru (2005). "Anatomy and histology of Virchow's node". Anatomical Science International. 80 (4): 193–8. doi:10.1111/j.1447-073X.2005.00114.x. PMID 16333915.
Further reading
- Cervin, J. R.; Silverman, J. F.; Loggie, B. W.; Geisinger, K. R. (1995). "Virchow's node revisited. Analysis with clinicopathologic correlation of 152 fine-needle aspiration biopsies of supraclavicular lymph nodes". Archives of pathology & laboratory medicine. 119 (8): 727–30. PMID 7646330.
- Negus, D.; Edwards, J. M.; Kinmonth, J. B. (1970). "Filling of cervical and mediastinal nodes from the thoracic duct and the physiology of virchow's node—studies by lymphography". British Journal of Surgery. 57 (4): 267–71. doi:10.1002/bjs.1800570407. PMID 5437920.
- Mizutani, Masaomi; Nawata, Shin-Ichi; Hirai, Ichiro; Murakami, Gen; Kimura, Wataru (2005). "Anatomy and histology of Virchow's node". Anatomical Science International. 80 (4): 193–8. doi:10.1111/j.1447-073X.2005.00114.x. PMID 16333915.