University of Pennsylvania Smell Identification Test
The University of Pennsylvania Smell Identification Test (UPSIT) is a test that is commercially available for smell identification to test the function of an individual's olfactory system. It has been administered to about 500,000 patients to this date. It is the gold standard of smell identification tests for its reliability (r=.94)[1] and practicality. Richard Doty invented UPSIT which has been used as a self-examination test in the diagnosis of many diseases including Parkinson's Disease and Alzheimer's. The test has been altered in several ways to be useful in different languages and cultures. There are also several trends that are found when UPSIT is administered based on demographics such as age, gender, history of smoking and other characteristics. [2]
Format
This test is a measurement of the individual's ability to detect odors at a suprathreshold level. The test is usually administered in a waiting room and takes only a few minutes. The test consists of 4 different 10 page booklets, with a total of 40 questions.[3] On each page, there is a different "scratch and sniff" strip which are embedded with a microencapsulated odorant. There is also a four choice multiple choice question on each page. The scents are released using a pencil. After each scent is released, the patient smells the level and detects the odor from the four choices. There is an answer column on the back of the test booklet, and the test is scored out of 40 items. The score is compared to scores in a normative database from 4000 normal individuals, this tells the level of absolute smell function.[1] The score also indicates how the patient does in accordance to their age group and gender.
The test is occasionally judged to have an American cultural bias. There are have been British, Chinese, French, German, Italian, Korean and Spanish UPSIT versions made.[4] There are also the Brief (Cross-Cultural) Smell Identification Test,[5] the Scandinavian Odor Identification Test.[6]
Olfactory system
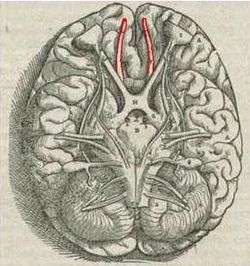
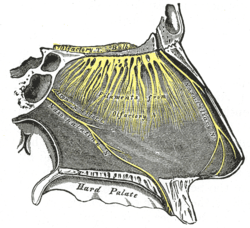
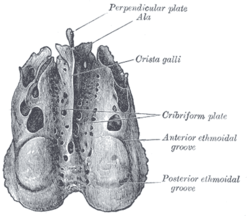
Through the nose, smell is induced when olfactory receptor cells are stimulated by volatile chemicals. The olfactory receptor cells, otherwise known as the primary olfactory neurons, are in the neuroepithilium. The neuroepithlium is located at the top of the nasal vault, which is at the upper portion of the nasal septum. The information received by the olfactory receptors is transmitted by the olfactory nerves to the olfactory bulb through the cribriform plate. In the olfactory bulb, olfactory nerves make synaptic contact with dendrites of mitral and tufted cells. Efferent neurons of the olfactory bulb become the fibers that form the olfactory tracts, which is directly under the frontal lobes in the brain. The axons from the mitral and tufted cells project this information to many other regions of the brain including the thalamus, hypothalamus and dorsolateral frontal cortex.[7]


The olfactory bulb has been said to be the olfactory thalamus. It performs the final stage of sensory processing before information is sent to the cortex. It has been proven that there is a strong correlation between cognitive function and olfactory function. It has been reported that the ability of detection of odors is not as challenging as the identification of odors. It has been hypothesized that this is due to lack of verbal or visual representations of odors.[8] It has also been speculated that olfactory function and odor detection have a correlation to memory function. It has been shown that olfactory identification is predictive of memory decline.[9]
Demographics
In general, women have a better sense of smell than men do.[10] This advantage can be observed very early on in childhood, even as early as 4 years of age. This is evidenced by several cultures. This superiority in women also increases with age. Overall, women have a higher functioning olfactory system than men do starting from a young age.
With the increase in age, there is an increased loss of the olfactory function. On average, individuals begin to lose function of their olfactory system by the age of 65. Of the individuals who do suffer a loss of olfactory function, half of the losses begin between the ages of 65 and 80. Also three quarters of these occur after the age of 80.[11] This plays a role in diagnosing Alzheimer's.
Genetics has been found to play a significant role in the ability of one's olfactory system as well.[12] If an individual does suffer from olfactory dysfunction, it is five times more likely that their first order relatives will also suffer from olfactory dysfunction.[13]
Smoking is also a major factor in a decrease of olfactory function. It can take years for past smokers to regain their presmoking olfactory function. Occasionally it is even impossible for individuals to regain this level in its entirety. The length of time it can take for smokers to regain this level depends on the duration and intensity of their smoking habits.[14]
The olfactory system can be compromised in several environments. This includes residents of large urban cities. Also, workers in certain industries, for example paper and chemical manufacturing industries.[15]
Diagnosis
There are many central nervous system disorders that are associated with olfactory dysfunction. Most of these dysfunctions classify as degenerative neuropsychiatric disorders. Some of these diseases are: Alzheimer's Disease, Parkinson's Disease, Huntington's Disease,[16] Korsakoff's Psychosis, Schizophrenia,[17] Congenital Anosmia,[18] Head Trauma,[19] Brain Tumors,[20] Acquired Immunodeficiency Syndrome(AIDS),[21] and Multiple Sclerosis.[22]
Alzheimer's
UPSIT has been used to detect Alzheimer's (AD). Smell loss can be a very early sign of detecting AD.[23] It has been suggested that AD affects odor identification and odor detection, this shows that AD patients have more trouble performing higher olfactory tasks that involve specific cognitive processes. During a functional magnetic resonance imaging (fMRI) study, blood oxygen level-dependent was found more strongly in control patients than AD patients, who showed a weaker signal.[24] It has also been found through several studies that olfactory function and cognition correlates to the severity of AD. Therefore, UPSIT is a very good clinical test to be able to determine the severity of AD.[8] During AD, a patient's olfactory bulb, amygdala and temporal cortices are affected. There is also severe nerve cell loss.
Parkinson's Disease
UPSIT is also used to diagnose Parkinson's Disease (PD). Smell dysfunction occurs in 90% of cases with PD. After the commercial release of UPSIT, there have been many studies published that have shown olfactory dysfunction in patients with PD. The many studies were undertaken because it was discovered that smell tests can differentiate PD from progressive supranuclear palsy, essential tremor, and parkinsonism induced by MPTP. It has been shown that the olfactory bulb is one of the two main regions where PD seems to begin. In families where there are individuals with PD, UPSIT can be used to predict whether other first degree relatives will also develop PD. It has been discovered that multiple factors contribute to the development of PD-related olfactory dysfunction.[25] As with AD, the UPSIT score can also determine the severity of PD. But people develop various levels of olfactory dysfunction. The disorders with the olfactory dysfunction are those with the most pathology, such as PD and AD.[25]
References
- 1 2 Doty, RL; Frye RE; Agrawal U (1989). "Internal consistency reliability of the fractionated and whole University of Pennsylvania Semll Identification Test.". Precept Psychophs. 45: 381–384. doi:10.3758/bf03210709.
- ↑ Doty, RL; Shaman P; Applebaum SL; et al. (1984). "Smell Identification ability: changes with age.". Science. 226: 1441–1443. doi:10.1126/science.6505700. PMID 6505700.
- ↑ Doty, R (2007). "Office procedures for quantitative assessment of olfactory function". American Journal of Rhinology. 24 (4): 460–473. doi:10.2500/ajr.2007.21.3043.
- ↑ Doty, RL (1995). The Smell Identification Test Administration Manual. Sensonics Inc. pp. 1–57.
- ↑ Doty, RL; Marcus A; Lee WW. (1996). "Development of the 12-item cross-cultural smell identification test (CC-SIT).". Laryngoscope. 106: 353–356. doi:10.1097/00005537-199603000-00021.
- ↑ Nordin, S; Bramerson A; Liden E; et al. (1999). "The Scandinavian Odor-Identification Test: Development, reliability, validity, and normative data.". Acta Otolaryngol. 118: 226–234. doi:10.1080/00016489850154946.
- ↑ Doty, Richard (2003). Handbook of Olfaction and Gustation. New York: Marcel Dekker, Inc. pp. 461–473.
- 1 2 Velaugudhan, L; Pritchard M; Powell J; Proitsi P; Lovestone S (July 2013). "Smell identification function as a severity and progression marker in Alzheimer's disease.". International Psychogeriatrics. 25 (7): 1157–1166. doi:10.1017/s1041610213000446.
- ↑ Swan, G.E.; Carmelli, D. (2002). "Impaired olfaction predicts cognitive decline in nondemented older adults". Neuroepidemiology. 21: 58–67. doi:10.1159/000048618.
- ↑ Liu, HC; Wang SJ; Lin KP; et al. (1995). "Performance on a smell screening test (the MODSIT): A study of 510 predominantly illiterate Chinese subjects". Physiological Behavior. 58: 1251–1255. doi:10.1016/0031-9384(95)02042-x.
- ↑ Ship, JA; Weiffenback JM (1993). "Age, gender, medical treatment and medication effects on smell identification.". Gerontol. 48: 26–32. doi:10.1093/geronj/48.1.m26.
- ↑ Roalf, DR; Turetsky BI; Owzar K; et al. (2006). "Unifhinal Olfactory function in schizophrenia patients and first degree relatives". J Neuropsychiatry Clinical Neuroscience. 18. 18: 389–396. doi:10.1176/jnp.2006.18.3.389.
- ↑ Segal, NL; Topolski TD; Wilson SM; et al. (1995). "Twin analysis of odor identification and perception.". Physiological Behavior. 57: 605–609. doi:10.1016/0031-9384(94)00328-3.
- ↑ Frye, RE; Schwartz BS; Doty RL (1990). "Dose-related effects of cigarette smoking on olfactory function". JAMA. 263: 1233–1236. doi:10.1001/jama.263.9.1233.
- ↑ Hirsch, AR; Zavala G. (1999). "Long-term effects on the olfactory system of exposure to hydrogen sulphide". Occupational and Environmental Medicine. 56: 284–287. doi:10.1136/oem.56.4.284.
- ↑ Bylsma, F.; Moberg, P.; Doty, R.; Brandt, J. (1997). "Odor identification in Huntington's disease patients and asymptomatic gene carriers.". The Journal of Neuropsychiatry and Clinical Neurosciences. 9: 598–600. doi:10.1176/jnp.9.4.598.
- ↑ Keshavan, M.; Montrose, D. Diwadkar, V. & Sweeney, J. (2009). "Olfactory identification in your relatives at risk for schizophrenia". Neuropsychiatric. 21: 121–124. doi:10.1111/j.1601-5215.2009.00390.x. Cite uses deprecated parameter
|coauthors=(help) - ↑ Amoore, JE (1967). "Specific anosmia: A clue to the olfactory code.". Nature. 214: 1095–1098. doi:10.1038/2141095a0.
- ↑ Yousem, D.; Geckle, R., Bilker, W., Kroger, H. Doty, R. (1999). "Posttraumatic smell loss: relationship of psychophysical tests and volumes of the olfactory bulbs and tracts and the temporal lobes.". Academic Radiology. 5. 6: 264–272. doi:10.1016/s1076-6332(99)80449-8. Cite uses deprecated parameter
|coauthors=(help) - ↑ Boldrey,, E.; Naffziger, H. Arnstein, L. (1950). "Signs and symptoms of supratentorial brain tumors in childhood.". The Journal of Pediatrics. 37: 463–468. doi:10.1016/s0022-3476(50)80255-x. Cite uses deprecated parameter
|coauthors=(help) - ↑ Vance, D. (2007). "Olfactory and psychomotor symptoms in HIV and aging: potential precursors to cognitive loss.". Medical Science Monitor: International Medical Journal of Experimental And Clinical Research. 13 (10).
- ↑ Hawkes, C.; Shephard B; Kobal G. (August 1997). "Assessment of Olfaction in multiple sclerosis: evidence of dysfunction by olfactory evoked response and identification tests.". Journal of Neurology, Neurosurgery, and Psychiatry. 63: 145–151. doi:10.1136/jnnp.63.2.145.
- ↑ Lange, R; Donathan, C.; Hughes, L. (2002). "Assessing olfactory abilities with the University of Pennsylvania smell identification test: a Rasch scaling approach.". Journal of Alzheimer's Disease. 4 (2): 77–91.
- ↑ Wang, J.; et al. (2010). "Olfactory deficit detected by fMRI in early Alzheimer's disease". Brain Research. 1357: 184–194. doi:10.1016/j.brainres.2010.08.018.
- 1 2 Doty, RL (June 2012). "Olfaction in Parkinson's disease and related disorders.". Neurobiology Of Disease. 3. 46: 527–552. doi:10.1016/j.nbd.2011.10.026.