Nursemaid's elbow
| Nursemaid's elbow | |
|---|---|
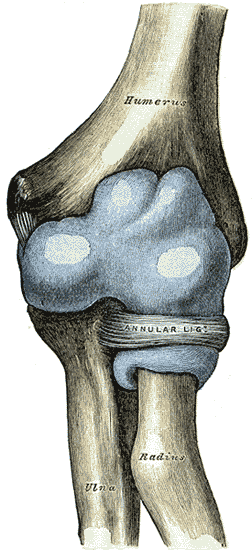 | |
| Capsule of elbow-joint (distended). Anterior aspect. (Nursemaid's elbow involves the head of radius slipping out from the anular ligament of radius.) | |
| Classification and external resources | |
| Specialty | emergency medicine |
| ICD-10 | S53.0 |
| ICD-9-CM | 832.0 |
| MedlinePlus | 000983 |
| eMedicine | emerg/392 |
Nursemaid's elbow, babysitter's elbow, or pulled elbow[1] is a dislocation of the elbow joint caused by a sudden pull on the extended pronated forearm, such as by an adult tugging on an uncooperative child or by swinging the child by the arms during play. The technical term for the injury is radial head subluxation.[2]
Overview
In radial head subluxation, there is little complaint of pain, and the patient generally reports pain in the proximal forearm. Radial head subluxation is a common pediatric presentation generally occurring between the ages of 1 and 3 years, although it can happen anytime between 6 months of age and 7 years. After age 3, children's joints and ligaments gradually grow stronger, making radial head subluxation less likely to occur. The etiology is slippage of the head of the radius under the annular ligament. The distal attachment of the annular ligament covering the radial head is weaker in children than in adults, allowing it to be more easily torn. The older child will usually point to the dorsal aspect of the proximal forearm when asked where it hurts. This may mislead one to suspect a buckle fracture of the proximal radius.[3] There is no tear in the soft tissue (probably due to the pliability of young connective tissues).[3]
This injury has also been reported in infants younger than six months and in older children up to the preteen years. There is a slight predilection for this injury to occur in girls and in the left arm. The classic mechanism of injury is longitudinal traction on the arm with the wrist in pronation, as occurs when the child is lifted up by the wrist. There is no support for the common assumption that a relatively small head of the radius as compared to the neck of the radius predisposes the young to this injury.
Anatomy
The forearm contains two bones: the radius and the ulna. These bones are attached to each other both at the proximal, or elbow, end and also at the distal, or wrist, end. Among other movements, the forearm is capable of pronation and supination, which is to say rotation about the long axis of the forearm. In this movement the ulna, which is connected to the humerus by a simple hinge-joint, remains stationary, while the radius rotates, carrying the wrist and hand with it. To allow this rotation, the proximal (elbow) end of the radius is held in proximity to the ulna by a ligament known as the annular ligament. This is a circular ligamentous structure within which the radius is free, with constraints existing elsewhere in the forearm, to rotate.The proximal end of the radius in young children is conical, with the wider end of the cone nearest the elbow. With the passage of time the shape of this bone changes, becoming more cylindrical but with the proximal end being widened.
If the forearm of a young child is pulled, it is possible for this traction to pull the radius into the annular ligament with enough force to cause it to be jammed therein. This causes significant pain, partial limitation of flexion/extension of the elbow and total loss of pronation/supination in the affected arm. The situation is rare in adults, or in older children, because the changing shape of the radius associated with growth prevents it.
Signs and symptoms
Radial head subluxation:
- The child stops using the arm, which is held in extension and pronated.[4]
- Minimal swelling.
- All movements are permitted except supination.
- Caused by longitudinal traction with the wrist in pronation, although in a series only 51% of patients were reported to have this mechanism, with 22% reporting falls, and patients less than 6 months of age noted to have the injury after rolling over in bed.
Treatment
To resolve the problem, the affected arm is moved in a way that causes the joint to move back into a normal position. The two main methods are hyperpronation and a combination of supination and flexion. In one study, hyperpronation required fewer attempts, was more successful initially, and was often successful when supination/flexion failed.[5]
See also
References
- ↑ Krul, Marjolein; Van Der Wouden, Johannes C; Van Suijlekom-Smit, Lisette WA; Koes, Bart W (2012). "Manipulative interventions for reducing pulled elbow in young children". Cochrane Database of Systematic Reviews. 1: CD007759. doi:10.1002/14651858.CD007759.pub3. PMID 22258973.
- ↑ Toupin, P; Osmond, M. H.; Correll, R; Plint, A (2007). "Radial head subluxation: How long do children wait in the emergency department before reduction?". CJEM. 9 (5): 333–7. PMID 17935648.
- 1 2 Nursemaid Elbow at eMedicine
- ↑ Radial Head Subluxation Joint Reduction at eMedicine
- ↑ MacIas, C. G.; Bothner, J.; Wiebe, R. (1998). "A Comparison of Supination/Flexion to Hyperpronation in the Reduction of Radial Head Subluxations". Pediatrics. 102 (1): e10. doi:10.1542/peds.102.1.e10. PMID 9651462.