Intrauterine device

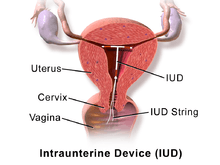
An intrauterine device (IUD or coil)[1] is a small contraceptive device, often 'T'-shaped, often containing either copper or levonorgestrel, which is inserted into the uterus. They are one form of long-acting reversible contraception which are the most effective types of reversible birth control.[2] Failure rates with the copper IUD is about 0.8% while the levonorgestrel IUD has a failure rate of 0.2% in the first year of use.[3] Among types of birth control they, along with birth control implants, result in the greatest satisfaction among users.[4] In 2007, IUDs were the most widely used form of reversible contraception, with more than 180 million users worldwide.[5]
Evidence supports effectiveness and safety in adolescents and those who have and have not previously had children.[4][6] IUDs do not affect breastfeeding and can be inserted immediately after delivery.[7] They may also be used immediately after an abortion.[8] Once removed, even after long-term use, fertility returns to normal immediately.[9]
While copper IUDs may increase menstrual bleeding and result in more painful cramps,[10] hormonal IUDs may reduce menstrual bleeding or stop menstruation altogether.[7] Cramping can be treated with NSAIDs.[11] Other potential complications include expulsion (2–5%) and rarely perforation of the uterus (less than 0.7%).[7][11] A previous model of the intrauterine device (the Dalkon shield) was associated with an increased risk of pelvic inflammatory disease; however, the risk is not affected with current models in those without sexually transmitted infections around the time of insertion.[12]
Types
The types of intrauterine devices available, and the names they go by, differ by location.
In the United States, there are two types available:[13]
- Nonhormonal copper IUD (ParaGard)
- IUD with progestogen (Mirena among others)
The WHO ATC labels both copper and hormonal devices as IUDs. In the United Kingdom, there are over 10 different types of copper IUDs available. In the UK, the term IUD refers only to these copper devices. Hormonal intrauterine contraception is considered to be a different type of birth control and is labeled with the term intrauterine system (IUS).[14][15]
Copper


Copper IUDs primarily work by disrupting sperm motility and damaging sperm so that they are prevented from joining with an egg. Copper acts as a spermicide within the uterus, increasing levels of copper ions, prostaglandins, and white blood cells within the uterine and tubal fluids.[10][16] The increased copper ions in the cervical mucus inhibit the sperm's motility and viability, preventing sperm from traveling through the cervical mucus, or destroying it as it passes through.[17] Copper can also alter the endometrial lining, but studies show that this alteration can prevent implantation, but not disrupt implantation.[18]
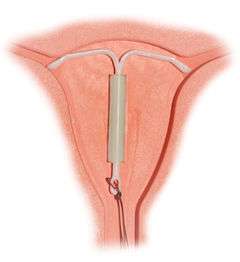
Most copper IUDs have a plastic T-shaped frame that is wound around with pure electrolytic copper wire and/or has copper collars (sleeves). The arms of the frame hold the IUD in place near the top of the uterus. The Paragard TCu 380a measures 32 mm (1.26") horizontally (top of the T), and 36 mm (1.42") vertically (leg of the T).
Copper IUDs have a first year failure rate ranging from 0.1 to 2.2%.[19]
In the Eurogine Gold T IUD,[20] which is made in Spain, there is a gold core, which further prevents the copper from fragmenting or corroding. GoldringMedusa is a differently-shaped German version of the Gold T.[21] Another form of AuCu IUD is called Goldlily which is made by the Hungarian company, Radelkis. Goldlily consists of a layer of copper wires wrapped around an original layer of gold wires, and it provides electrochemical protection in addition to ionic protection.[22]
Silver IUDs also exist. Radelkis also makes Silverlily, which is similar to Goldlily, and GoldringMedusa is available in an AgCu version as well. Nova-T 380 contains a strengthening silver core, but does not incorporate silver ions themselves to provide electrochemical protection.[14][23] Other shapes of IUD include the so-called U-shaped IUDs, such as the Load and Multiload, and the frameless IUD that holds several hollow cylindrical minuscule copper beads. It is held in place by a suture (knot) to the fundus of the uterus. It is mainly available in China, Europe, and Germany, although some clinics in Canada can provide it. A framed copper IUD called the IUB SCu300 coils during deployment to form a three dimensional spherical shape and is based on a nickel titanium shape memory alloy core.[24]
In addition to copper, noble metal and progestogen IUDs, patients in China can get copper IUDs with indomethacin. This non-hormonal compound reduces the severity of menstrual bleeding, and these coils are popular.[25]
Advantages of the copper IUD include its ability to provide emergency contraception up to five days after unprotected sex. It is the most effective form of emergency contraception available.[26] It works by preventing fertilization or implantation; however does not affect already implanted embryos.[18] It contains no hormones, so it can be used while breastfeeding, and fertility returns quickly after removal.[27] Copper IUDs are also available in a wider range of sizes and shapes than hormonal IUDs.
Disadvantages include the possibility of heavier menstrual periods and more painful cramps.[10]
Hormonal

Hormonal IUDs (brand names Mirena, Skyla, and Liletta; referred to as intrauterine systems in the UK) work by releasing a small amount of levonorgestrel, a progestin. The primary mechanism of action is making the inside of the uterus fatal to sperm.[28] They can also thin the endometrial lining and potentially impair implantation but this is not their usual function.[29][30] Because they thin the endometrial lining, they reduce or even prevent menstrual bleeding, and can be used to treat menorrhagia (heavy menses), once pathologic causes of menorrhagia (such as uterine polyps) have been ruled out.[31]
The progestin released by hormonal IUDs primarily acts locally; use of Mirena results in much lower systemic progestin levels than other very-low-dose progestogen only contraceptives.[32]
Mirena is approved for use up to five years in the US, though studies support its efficacy for up to seven years.[33] Skyla uses the same mechanism of action, but is smaller and releases a lower dose of levonorgestrel, and is only approved for up to three years. Liletta is more similar to Mirena in both shape and dose of levonorgestrel released; it has currently been approved for usage up to three years.[34]
Inert
Inert IUDs are IUDs with no bioactive components; they are made of inert materials like stainless steel (such as the stainless steel ring, or SSR, a flexible ring of steel coils that can deform to be pushed through the cervix) or plastic (such as the Lippes Loop, which can be inserted through the cervix in a cannula and takes a trapezoidal shape within the uterus). They are less effective than copper or hormonal IUDs, with a side effect profile similar to copper IUDs. Their primary mechanism of action is inducing a local foreign body reaction, which makes the uterine environment hostile both to sperm and to implantation of an embryo.[35] They may have higher rates of preventing pregnancy after fertilization, instead of before fertilization, compared to copper or hormonal IUDs.[36]
No inert IUDs are approved for use by the healthcare authorities in the United States, UK, or Canada. In China, where IUDs are the most common form of contraception, copper IUD production replaced inert IUD production in 1993.[37] However, as of 2008, the most common IUD used by immigrants presenting to Canadian clinics for removal of IUDs placed in China was still the SSR. As the SSR has no string for removal, it can present a challenge to healthcare providers unfamiliar with IUD types not available in their region.[38]
Adverse effects

Regardless of containing progestogen or copper, potential side effects of intrauterine devices include expulsion, uterus perforation, pelvic inflammatory disease (especially in the first 21 days after insertion), as well as irregular menstrual pattern. A small probability of pregnancy remains after IUD insertion, and when it occurs there is a greater risk of ectopic pregnancy.
Substantial pain that needs active management occurs in approximately 17% of nulliparous women and approximately 11% of parous women.[39] In such cases, NSAID are evidenced to be effective.[39] However, no prophylactic analgesic drug have been found to be effective for routine use for women undergoing IUD insertion.[39]
Also, IUDs with progestogen confer an increased risk of ovarian cysts,[40] and IUDs with copper confer an increased risk of heavier periods.
Menstrual Cup companies recommend that women with IUDs who are considering using menstrual cups should consult with their gynecologists before use. There have been rare cases in which women using IUDs dislodged them when removing their menstrual cups, however, this can also happen with tampon use.[41]
Mechanism
IUDs primarily work by preventing fertilization.[42] The progestogen released from the hormonal IUDs may prevent ovulation from occurring but only partially.[43][44] The hormone also thickens the cervical mucus so that sperm cannot reach the fallopian tubes. The copper IUDs contain no hormones, but the copper ions in the cervical mucus are toxic to sperm. They also cause the uterus and fallopian tubes to produce a fluid that contains white blood cells, copper ions, enzymes, and prostaglandins, a combination that is also toxic to sperm.[43] The very high effectiveness of copper-releasing IUDs as emergency contraceptives implies they may also act by preventing implantation of the blastocyst.[45][46] In non-emergency use, prevention of implantation is at most an exceptional method of action, not a typical mechanism of action.[17]
History
The history of intrauterine devices dates back to the early 1900s. Unlike IUDs, early interuterine devices crossed both the vagina and the uterus, causing a high rate of pelvic inflammatory disease in a time period when gonorrhea was more common. The first IUD was developed in 1909 by the German physician, Richard Richter of Waldenburg. His device was made of silkworm gut and was not widely used.[47]
Ernst Gräfenberg, another German physician after whom the G-spot is named, created the first Ring IUD, Gräfenberg's ring, made of silver filaments. His work was suppressed during the Nazi regime, when contraception was considered a threat to Aryan women.[47] He moved to the United States, where his colleagues H. Hall and M. Stone took up his work after his death and created the stainless steel Hall-Stone Ring. A Japanese doctor named Tenrei Ota also developed a silver or gold IUD called the Precea or Pressure Ring.[47]
Jack Lippes helped begin the increase of IUD use in the United States in the late 1950s. In this time, thermoplastics, which can bend for insertion and retain their original shape, became the material used for first-generation IUDs. Lippes also devised the addition of the monofilament nylon string, which facilitates IUD removal. His trapezoid shape Lippes Loop IUD became one of the most popular first-generation IUDs. In the following years, many different shaped plastic IUDs were invented and marketed.[47] These included the infamous Dalkon Shield, whose poor design caused bacterial infection and led to thousands of lawsuits. Although the Dalkon shield was removed from the market, it had a lasting, negative impact on IUD use and reputation in the United States.[48] Lazar C. Margulies developed the first plastic IUD using thermoplastics in the 1960s.[49] His innovation allowed insertion of the IUD into the uterus without the need to dilate the cervix.[50]
The invention of the copper IUD in the 1960s brought with it the capital 'T' shaped design used by most modern IUDs. U.S. physician Howard Tatum determined that the 'T' shape would work better with the shape of the uterus, which forms a 'T' when contracted. He predicted this would reduce rates of IUD expulsion.[47] Together, Tatum and Chilean physician Jaime Zipper discovered that copper could be an effective spermicide and developed the first copper IUD, TCu200. Improvements by Tatum led to the creation of the TCu380A (ParaGard), which is currently the preferred copper IUD.[47]
The hormonal IUD was also invented in the 1960s and 1970s; initially the goal was to mitigate the increased menstrual bleeding associated with copper and inert IUDs. The first model, Progestasert, was conceived of by Antonio Scommengna and created by Tapani J. V. Luukkainen, but the device only lasted for one year of use.[48] Progestasert was manufactured until 2001.[51] One commercial hormonal IUD which is currently available, Mirena, was also developed by Luukkainen and released in 1976.[47] The manufacturer of the Mirena, Bayer AG, became the target of multiple lawsuits over allegations that Bayer failed to adequately warn users that the IUD could pierce the uterus and migrate to other parts of the body.[52]
References
- ↑ "IUD (intrauterine device)". Contraception guide. NHS Choices. Retrieved 2 March 2014.
the intrauterine device, or IUD (sometimes called a coil)
- ↑ Winner, B; Peipert, JF; Zhao, Q; Buckel, C; Madden, T; Allsworth, JE; Secura, GM. (2012). "Effectiveness of Long-Acting Reversible Contraception". New England Journal of Medicine. 366 (21): 1998–2007. doi:10.1056/NEJMoa1110855. PMID 22621627.
- ↑ Hurt, K. Joseph (eds.); et al. (2012-03-28). The Johns Hopkins manual of gynecology and obstetrics. (4th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 232. ISBN 978-1-60547-433-5.
- 1 2 Committee on Adolescent Health Care Long-Acting Reversible Contraception Working Group, The American College of Obstetricians and, Gynecologists (October 2012). "Committee opinion no. 539: adolescents and long-acting reversible contraception: implants and intrauterine devices.". Obstetrics and gynecology. 120 (4): 983–8. doi:10.1097/AOG.0b013e3182723b7d. PMID 22996129.
- ↑ Darney, Leon Speroff, Philip D. (2010). A clinical guide for contraception (5th ed.). Philadelphia, Pa.: Lippincott Williams & Wilkins. pp. 242–243. ISBN 9781608316106.
- ↑ Black, K; Lotke, P.; Buhling, K.J.; Zite, N.B.; et al. (Intrauterine contraception for Nulliparous women: Translating Research into Action (INTRA), group) (October 2012). "A review of barriers and myths preventing the more widespread use of intrauterine contraception in nulliparous women". The European Journal of Contraception & Reproductive Health Care. 17 (5): 340–50. doi:10.3109/13625187.2012.700744. PMID 22834648.
- 1 2 3 Gabbe, Steven (2012). Obstetrics: Normal and Problem Pregnancies. Elsevier Health Sciences. p. 527. ISBN 9781455733958.
- ↑ Steenland, MW; Tepper, NK; Curtis, KM; Kapp, N (November 2011). "Intrauterine contraceptive insertion postabortion: a systematic review.". Contraception. 84 (5): 447–64. doi:10.1016/j.contraception.2011.03.007. PMID 22018119.
- ↑ Hurd, [edited by] Tommaso Falcone, William W. (2007). Clinical reproductive medicine and surgery. Philadelphia: Mosby. p. 409. ISBN 9780323033091.
- 1 2 3 Grimes, D.A., MD (2007). Hatcher, R.A.; Nelson, T.J.; Guest, F.; Kowal, D., eds. "Intrauterine Devices (IUDs)". Contraceptive Technology (19th ed.). New York: Ardent Media.
- 1 2 Marnach, ML; Long, ME; Casey, PM (March 2013). "Current issues in contraception.". Mayo Clinic proceedings. Mayo Clinic. 88 (3): 295–9. doi:10.1016/j.mayocp.2013.01.007. PMID 23489454.
- ↑ Sonfield, Adam (Fall 2007). "Popularity Disparity: Attitudes About the IUD in Europe and the United States". Guttmacher Policy Review. Guttmacher Institute. Retrieved 2016-06-04.
- ↑ Treiman K, Liskin L, Kols A, Rinehart W (1995), "IUDs – an update" (PDF), Popul Rep B (6): 1–35, PMID 8724322, retrieved 2006-01-01
- 1 2 "Contraceptive coils (IUDs)". NetDoctor.co.uk. 2006. Retrieved 2006-07-05.
- ↑ French R, Van Vliet H, Cowan F, et al. (2004). Sorhaindo AM, ed. "Hormonally impregnated intrauterine systems (IUSs) versus other forms of reversible contraceptives as effective methods of preventing pregnancy". Cochrane Database of Systematic Reviews (3): CD001776. doi:10.1002/14651858.CD001776.pub2. PMID 15266453.
- ↑ "Mechanisms of the Contraceptive Action of Hormonal Methods and Intrauterine Devices (IUDs)". Family Health International. 2006. Retrieved 2006-07-05.
- 1 2 Oritz ME, Croxatto HB (2007). "Copper-T intrauterine device and levonorgestrel intrauterine system: biological bases of their mechanism of action". Contraception. 75 (6 Suppl): S16–S30. doi:10.1016/j.contraception.2007.01.020. PMID 17531610.
- 1 2 "Facts are Important: Emergency Contraception (EC) and Intrauterine Devices (IUDs) are Not Abortifacients" (PDF). American Congress of Obstetricians and Gynecologists. June 12, 2014. Retrieved July 14, 2015.
Copper ions released from the IUD create an environment that is toxic to sperm, preventing fertilization.14 Copper can also alter the endometrial lining, but studies show that this alteration can prevent implantation, but not disrupt implantation
- ↑ Kulier R, O'Brien PA, Helmerhorst FM, Usher-Patel M, D'Arcangues C (2007), "Copper containing, framed intra-uterine devices for contraception", Cochrane Database Syst Rev (4): CD005347, doi:10.1002/14651858.CD005347.PUB3, PMID 17943851
- ↑ http://www.eurogine.com
- ↑ http://www.viomed.de/de/medusa
- ↑ http://www.radelkis.hu/en/orvos/huv/frames.html
- ↑ Schering (May 13, 2003). "Nova T380 Patient information leaflet (PIL)". Retrieved 2007-04-27.
- ↑ Baram I, Weinstein A, Trussell J (February 2014), "The IUB, a newly invented IUD: a brief report", Contraception, 89 (2): 139–141, doi:10.1016/j.contraception.2013.10.017, PMID 24309220
- ↑ Li Y, Zhang SM, Chen F, et al. (December 2011). "[A multi-center randomized controlled trial of intrauterine device use in Chinese women]". Zhonghua Yi Xue Za Zhi (in Chinese). 91 (45): 3172–5. PMID 22333096.
- ↑ Cleland K, Zhu H, Goldstuck N, Cheng L, Trussell J (July 2012), "The efficacy of intrauterine devices for emergency contraception: a systematic review of 35 years of experience", Hum. Reprod., 27 (7): 1994–2000, doi:10.1093/humrep/des140, PMID 22570193
- ↑ Belhadj H, Sivin I, Diaz S, et al. (September 1986), "Recovery of fertility after use of the levonorgestrel 20 mcg/d or Copper T 380 Ag intrauterine device", Contraception, 34 (3): 261–7, doi:10.1016/0010-7824(86)90007-7, PMID 3098498
- ↑ Speroff, Leon; Darney, Philip D. (2011). "Intrauterine contraception". A clinical guide for contraception (5th ed.). Philadelphia: Lippincott Williams & Wilkins. pp. 239–280. ISBN 978-1-60831-610-6. pp. 246–247:
Mechanism of action
The contraceptive action of all IUDs is mainly in the intrauterine cavity. Ovulation is not affected, and the IUD is not an abortifacient.58–60 It is currently believed that the mechanism of action for IUDs is the production of an intrauterine environment that is spermicidal.
Nonmedicated IUDs depend for contraception on the general reaction of the uterus to a foreign body. It is believed that this reaction, a sterile inflammatory response, produces tissue injury of a minor degree but sufficient enough to be spermicidal. Very few, if any, sperm reach the ovum in the fallopian tube.
The progestin-releasing IUD adds the endometrial action of the progestin to the foreign body reaction. The endometrium becomes decidualized with atrophy of the glands.65 The progestin IUD probably has two mechanisms of action: inhibition of implantation and inhibition of sperm capacitation, penetration, and survival. - ↑ ESHRE Capri Workshop, Group (2008). "Intrauterine devices and intrauterine systems.". Human Reproduction Update. 14 (3): 197–208. doi:10.1093/humupd/dmn003. PMID 18400840.
Both copper IUDs and levonorgestrel releasing IUSs may interfere with implantation
- ↑ Hatcher, Robert A. (2011). Contraceptive technology (20th rev. ed.). [New York, N.Y.]: Ardent Media. p. 162. ISBN 978-1-59708-004-0.
Although the precise mechanism of action is not known, currently available IUCs work primarily by preventing sperm from fertilizing ova.26 IUCs are not abortifacients: they do not interrupt an implanted pregnancy.27 Pregnancy is prevented by a combination of the "foreign body effect" of the plastic or metal frame and the specific action of the medication (copper or levonorgestrel) that is released. Exposure to a foreign body causes a sterile inflammatory reaction in the intrauterine environment that is toxic to sperm and ova and impairs implantation.28,29 The production of cytotoxic peptides and activation of enzymes lead to inhibition of sperm motility, reduced sperm capacitation and survival, and increased phagocytosis of sperm.30,31… The progestin in the LNg IUC enhances the contraceptive action of the device by thickening cervical mucus, suppressing the endometrium, and impairing sperm function. In addition, ovulation is often impaired as a result of systemic absorption of levonorgestrel
- ↑ Luis Bahamondes; M Valeria Bahamondes; Ilza Monteiro. (2008), "Levonorgestrel-releasing intrauterine system: uses and controversies.", Expert Review of Medical Devices, 4: 437–45, doi:10.1586/17434440.5.4.437, PMID 18573044
- ↑ Malik S (January 2013). "Levonorgestrel-IUS system and endometrial manipulation". J Midlife Health. 4 (1): 6–7. doi:10.4103/0976-7800.109625. PMC 3702070
 . PMID 23833526.
. PMID 23833526. - ↑ Sivin I, Stern J, Coutinho E, et al. (November 1991). "Prolonged intrauterine contraception: a seven-year randomized study of the levonorgestrel 20 mcg/day (LNg 20) and the Copper T380 Ag IUDS". Contraception. 44 (5): 473–80. doi:10.1016/0010-7824(91)90149-a. PMID 1797462.
- ↑ "Liletta - A Third Levonorgestrel-Releasing IUD". The Medical Letter on Drugs and Therapies. 57: 99–100. July 6, 2015. PMID 26147893. Retrieved Oct 6, 2015.
- ↑ Ortiz, ME; Croxatto HB (June 2007). "Copper-T intrauterine device and levonorgestrel intrauterine system: biological bases of their mechanism of action.". Contraception. 75 (6): S16–30. doi:10.1016/j.contraception.2007.01.020. PMID 17531610.
- ↑ ESHRE Capri Workshop Group (April 2008). "Intrauterine devices and intrauterine systems". Human Reproduction Update. 14 (3): 197–208. doi:10.1093/humupd/dmn003. PMID 18400840.
- ↑ Bilian X (June 2007). "Chinese experience with intrauterine devices". Contraception. 75 (6 Suppl): S31–4. doi:10.1016/j.contraception.2006.12.007. PMID 17531613.
- ↑ Cheung VY (June 2010). "A 10-year experience in removing Chinese intrauterine devices". Int J Gynaecol Obstet. 109 (3): 219–22. doi:10.1016/j.ijgo.2009.12.018. PMID 20219193.
- 1 2 3 Gemzell-Danielsson, K.; Mansour, D.; Fiala, C.; Kaunitz, A. M.; Bahamondes, L. (2013). "Management of pain associated with the insertion of intrauterine contraceptives". Human Reproduction Update. 19 (4): 419–427. doi:10.1093/humupd/dmt022.
- ↑ Bahamondes L; Hidalgo M; Petta CA; Diaz J; Espejo-Arce X; Monteiro-Dantas C. (2003), "Enlarged ovarian follicles in users of a levonorgestrel-releasing intrauterine system and contraceptive implant", J. Reproduc. Med., 48 (8): 637–640, PMID 12971147
- ↑ "Menstrual Cup use and IUDs". Feminine Wear. Retrieved 22 December 2013.
- ↑ Steven G. Gabbe; et al. (eds.). Obstetrics : normal and problem pregnancies (6th ed.). Philadelphia: Elsevier/Saunders. p. 528. ISBN 9781437719352.
- 1 2 http://center4research.org/medical-care-for-adults/birth-control/understanding-the-iud/
- ↑ http://www.mayoclinic.org/tests-procedures/mirena/basics/definition/prc-20012867
- ↑ Trussell, James; Schwarz, Eleanor Bimla (2011). "Emergency contraception". In Hatcher, Robert A.; Trussell, James; Nelson, Anita L.; Cates, Willard Jr.; Kowal, Deborah; Policar, Michael S. Contraceptive technology (20th revised ed.). New York: Ardent Media. pp. 113–145. ISBN 978-1-59708-004-0. ISSN 0091-9721. OCLC 781956734. p. 121:
Mechanism of action
Copper-releasing IUCs
When used as a regular or emergency method of contraception, copper-releasing IUCs act primarily to prevent fertilization. Emergency insertion of a copper IUC is significantly more effective than the use of ECPs, reducing the risk of pregnancy following unprotected intercourse by more than 99%.2,3 This very high level of effectiveness implies that emergency insertion of a copper IUC must prevent some pregnancies after fertilization.
Emergency contraceptive pills
To make an informed choice, women must know that ECPs—like the birth control pill, patch, ring, shot, and implant,76and even like breastfeeding77—prevent pregnancy primarily by delaying or inhibiting ovulation and inhibiting fertilization, but may at times inhibit implantation of a fertilized egg in the endometrium. However, women should also be informed that the best available evidence indicates that ECPs prevent pregnancy by mechanisms that do not involve interference with post-fertilization events.
ECPs do not cause abortion78 or harm an established pregnancy. Pregnancy begins with implantation according to medical authorities such as the US FDA, the National Institutes of Health79 and the American College of Obstetricians and Gynecologists (ACOG).80
Ulipristal acetate (UPA). One study has demonstrated that UP can delay ovulation.81... Another study found that UPA altered the endometrium, but whether this change would inhibit implantation is unknown.82
p. 122:
Progestin-only emergency contraceptive pills. Early treatment with ECPs containing only the progestin levonorgestrel has been show to impair the ovulatory process and luteal function.83–87
p. 123:
Combined emergency contraceptive pills. Several clinical studies have shown that combined ECPs containing ethinyl estradiol and levonorgestrel can inhibit or delay ovulation.107–110 - ↑ RCOG Faculty of Sexual; Reproductive Healthcare; Clinical Effectiveness Unit (January 2012). Clinical guidance: emergency contraception (PDF). London: Royal College of Obstetricians and Gynaecologists. ISSN 1755-103X. Retrieved 2012-04-30.p.3:
How does EC work?
In 2002, a judicial review ruled that pregnancy begins at implantation, not fertilisation.8 The possible mechanisms of action should be explained to the patient as some methods may not be acceptable, depending on individual beliefs about the onset of pregnancy and abortion.
Copper-bearing intrauterine device (Cu-IUD). Copper is toxic to the ovum and sperm and thus the copper-bearing intrauterine device (Cu-IUD) is effective immediately after insertion and works primarily by inhibiting fertilisation.9–11 A systematic review on mechanisms of action of IUDs showed that both pre- and postfertilisation effects contribute to efficacy.11If fertilisation has already occurred, it is accepted that there is an anti-implantation effect,12,13
Levonorgestrel (LNG). The precise mode of action of levonorgestrel (LNG) is incompletely understood but it is thought to work primarily by inhibition of ovulation.16,17
Ulipristal acetate (UPA). UPA’s primary mechanism of action is thought to be inhibition or delay of ovulation.2 - 1 2 3 4 5 6 7 Thiery, Michel (March 1997). "Pioneers of the intrauterine device" (PDF). European Journal of Contraception and Reproductive Health Care. 2 (1): 15–23. doi:10.1080/13625189709049930. PMID 9678105. Archived from the original (PDF) on August 20, 2006.
- 1 2 Thiery M (June 2000), "Intrauterine contraception: from silver ring to intrauterine contraceptive implant", Eur. J. Obstet. Gynecol. Reprod. Biol., 90 (2): 145–52, doi:10.1016/s0301-2115(00)00262-1, PMID 10825633
- ↑ Thiery, M. (March 1997). "Pioneers of the Intrauterine Device" (PDF). The European Journal of Contraception and Reproductive Health Care. The Parthenon Publishing Group. 2 (1). Archived from the original (PDF) on 20 August 2006. Retrieved 24 March 2016.
- ↑ Reed, James (1984). The Birth Control Movement and American Society: From Private Vice to Public Virtue. Princeton University Press. p. 306. ISBN 9781400856596.
- ↑ Smith (pseudonym), Sydney (March 8, 2003). "Contraceptive Concerns". medpundit: Commentary on medical news by a practicing physician. Retrieved 2006-07-16.
- ↑ http://newsandinsight.thomsonreuters.com/Legal/News/2013/05_-_May/Judge_calls_for_female_lawyers_on_plaintiffs__committee_in_Mirena_MDL/
| Oral |
| -solution.jpg)     | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ophthalmic, otologic, nasal |
| |||||||||||||||||||||||||||||||||
| Urogenital | ||||||||||||||||||||||||||||||||||
| Rectal (enteral) | ||||||||||||||||||||||||||||||||||
| Dermal |
| |||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||